
In 2020, an estimated 5.8 million individuals used paid long-term providers and helps (LTSS) delivered in residence and neighborhood settings and 1.9 million used LTSS delivered in institutional settings, in accordance with CBO estimates. Most individuals ages 65 and older and many individuals below age 65 with disabilities have Medicare, however Medicare doesn’t cowl most LTSS and as a substitute, Medicaid is the first payer for LTSS. To qualify for protection of LTSS below Medicaid, individuals should meet state-specific eligibility necessities concerning their ranges of revenue, wealth, and useful limitations. An unknown, however most likely even bigger variety of individuals, used unpaid LTSS that’s offered by household, mates, or neighbors. LTSS embody the broad vary of paid and unpaid medical and private care providers that help with actions of each day dwelling (resembling consuming, bathing, and dressing) and instrumental actions of each day dwelling (resembling making ready meals, managing remedy, and housekeeping). They’re offered to individuals who want such providers due to getting old, power sickness, or incapacity, and embody nursing facility care, grownup daycare packages, residence well being aide providers, private care providers, transportation, and supported employment. These providers could also be offered over a interval of a number of weeks, months, or years, relying on a person’s well being care protection and stage of want.
There have been longstanding challenges discovering sufficient staff to offer LTSS for all individuals who want such providers, and the COVID-19 pandemic exacerbated these points significantly. In response to the pandemic, the federal government promulgated new initiatives to assist enhance security and high quality in nursing services, and created the first-ever set of high quality measures for residence and community-based providers (HCBS), however these steps are unlikely to handle long-standing challenges in financing and offering LTSS. The federal authorities additionally offered states with non permanent authorities and funding to offer new or further LTSS in the course of the pandemic, however these authorities and funding are time-limited. Because the inhabitants ages and as advances in drugs and expertise allow individuals with critical disabilities to dwell longer, the variety of individuals in want of LTSS is anticipated to develop. Wanting ahead, there’ll doubtless be continued curiosity amongst policymakers in increasing the provision of LTSS and bettering their high quality, although figuring out the sources to take action shall be difficult.
1. With over one-fifth of all U.S. COVID-19 deaths taking place in long-term care services, the pandemic highlighted ongoing points with LTSS.
Over 209,000 COVID-19 deaths, or simply over each one in 5 COVID-19 deaths, has been in a long-term care facility (together with nursing properties, assisted dwelling services, ICF/IIDs, and different settings) (Determine 1). These deaths highlighted many ongoing challenges for such services together with quickly rising demand for LTSS that outpaced out there sources, employee shortages, improper an infection management measures, and isolation amongst individuals dwelling in establishments. In early 2022, the Biden Administration introduced new initiatives centered on bettering nursing facility care high quality, oversight, knowledge transparency, profession pathways, and pandemic and emergency preparedness. Key coverage proposals embody establishing minimal staffing ranges for Medicare and Medicaid-certified nursing services, strengthening oversight of poor-performing nursing services, supporting state efforts to tie Medicaid reimbursement charges to will increase in employees compensation, and launching a nationwide nursing profession pathways marketing campaign to recruit, practice, and retain long-term care employees, amongst others. In August 2022, the administration additionally launched a brand new research to tell minimal staffing necessities for nursing properties. A number of states additionally enacted vaccine mandates for nursing residence staff. Early proof means that these mandates resulted in larger charges of vaccination amongst employees with none improve within the frequency of reported staffing shortages.
2. LTSS are extraordinarily costly and never lined by Medicare.
In 2021, the median annual prices of care within the U.S. had been $108,405 for a non-public room in a nursing residence, $54,000 for an assisted dwelling facility, and $61,776 for a house well being aide prices (Determine 2). These prices characterize what individuals could be anticipated to pay if they didn’t qualify for Medicaid. (A small variety of individuals have non-public long-term care insurance coverage, which helps defray these prices.) Nursing facility prices had been larger than the prices of different providers however many individuals dwelling exterior of nursing services use a number of providers concurrently. Virtually all LTSS prices exceeded the median revenue for Medicare beneficiaries in 2019. The prices of 1 yr of nursing facility care exceeded the median financial savings for Medicare beneficiaries in 2019 ($73,800), which means over half of individuals on Medicare don’t have ample financial savings to pay for one yr of nursing facility care.
Medicare gives residence well being and expert nursing facility care below particular circumstances, however the Medicare profit is taken into account “post-acute” care and customarily not out there for individuals needing providers on an ongoing foundation. There are 8.0 million Medicare beneficiaries who meet the revenue, wealth, and well being necessities for Medicaid and are enrolled each packages (generally known as “twin eligibles”). (A further 3.3 million Medicare beneficiaries are enrolled in Medicaid however solely obtain protection of Medicare premiums and in some circumstances, value sharing.) For Medicaid-Medicare enrollees with full Medicaid advantages, Medicare is the first payer for acute and post-acute care providers and Medicaid covers ongoing LTSS. Medicaid performs a key function in affordability and entry to LTSS for individuals who qualify as a result of LTSS prices could also be troublesome for individuals to afford when paying out-of-pocket. In some circumstances, individuals solely qualify for Medicaid after exhausting their financial savings on the prices of LTSS. The share of Medicare beneficiaries who’re enrolled in Medicaid varies extensively by state. Such variation displays variations in state coverage, and within the revenue and wealth distribution of Medicare beneficiaries throughout the states.
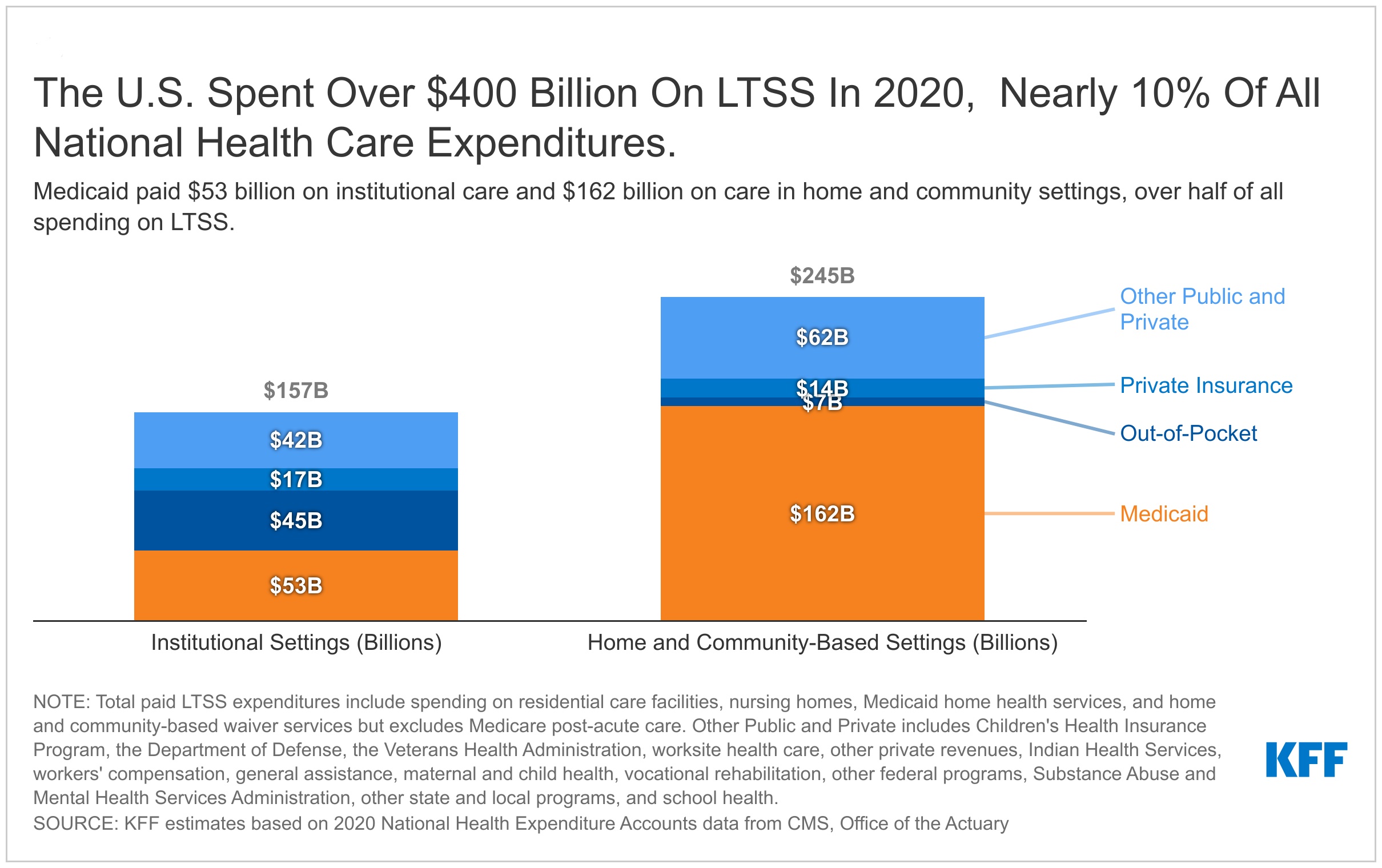
3. The U.S. spent over $400 billion on LTSS in 2020, almost 10% of all Nationwide Well being Care Expenditures.
In 2020, Medicaid paid 54% of the over $400 billion spent on LTSS within the U.S., individuals paid a further 13% out-of-pocket, non-public insurance coverage paid 8%, and different private and non-private payers paid the remaining 26%. Residence and community-based providers (HCBS) embody residential care services, Medicaid residence well being providers, and Medicaid HCBS waiver providers. Spending on these providers was $245 billion and the remaining $157 billion was spent on institutional LTSS resembling nursing facility care (Determine 3). These totals exclude $86 billion in Medicare spending on post-acute care, and spending on residence well being that was paid out-of-pocket ($13 billion), by non-public well being insurers ($16 billion), and by different private and non-private payers ($14 billion). These estimates exclude spending on residence well being by payers aside from Medicaid as a result of most providers in that class are acute care resembling sturdy medical gear offered at residence or care following a serious surgical procedure or hospitalization. Medicaid residence well being spending consists of each acute care and LTSS, however it’s doubtless that the majority residence well being is offered on an ongoing foundation within the Medicaid program. The institutional spending numbers exclude the room and board prices related to assisted dwelling services, that are thought of home-based settings. The providers delivered in assisted dwelling services, resembling residence well being and private care, could be thought of HCBS and lined below Medicaid as residence well being and private care advantages.
4. Greater than half of LTSS spending pays for residence and community-based providers, however there’s great variation throughout states.
LTSS could also be offered in numerous settings which are broadly categorized as institutional or non-institutional. Institutional settings embody nursing services and intermediate care services for individuals with mental disabilities. Companies offered in non-institutional settings are often known as residence and community-based providers (HCBS), and these settings might embody an individual’s residence, grownup day care facilities, assisted dwelling settings, and group properties. Federal Medicaid statutes require states to cowl institutional LTSS and residential well being, however the the rest of HCBS are non-compulsory. Even with no mandate to cowl HCBS, Medicaid LTSS spending has shifted from institutional to non-institutional settings over time. That shift displays beneficiary preferences for receiving care in non-institutional settings and necessities for states to offer providers within the least restrictive setting attainable stemming from the Olmstead choice In most states, a minimum of half—and infrequently considerably greater than half—of LTSS spending was on HCBS in Fiscal Yr 2019. Nonetheless, there’s substantial state variation within the share of Medicaid LTSS expenditures which are spent on HCBS, starting from 33% in Mississippi to 83% in Oregon. 4 states (Oregon, Minnesota, Arizona, and New Mexico) spent over 75% of their whole Medicaid LTSS spending on HCBS, whereas 18 states spent below 50% (Determine 4).
5. Most Medicaid LTSS spending is for people who find themselves ages 65 and over or who’re below age 65 with disabilities.
The overwhelming majority of Medicaid LTSS spending is amongst those that are 65 or older or below age 65 and eligible for Medicaid on the premise of incapacity (Determine 5). In CY 2019, such enrollees comprised almost 95% of fee-for-service (FFS) LTSS spending however lower than 25% of enrollment. These totals embody spending on institutional and non-institutional care, however exclude spending paid for by managed care plans. Though the vast majority of LTSS continues to be paid for immediately by states, the usage of managed care to offer LTSS has elevated over time. Below managed LTSS, states pay premiums to managed care plans and people plans pay for the well being care and LTSS that enrollees use. Medicaid administrative knowledge present how a lot states are spending on the premiums, however don’t typically present how a lot the managed care plans are spending on well being care and LTSS. Because of this, it’s troublesome to apportion the prices of premiums throughout well being care and LTSS.
6. Enrollees ages 65 and older or below age 65 with disabilities have larger general Medicaid prices.
Medicaid’s per individual spending for people who find themselves 65 or older or below age 65 with disabilities is considerably larger than it’s for different enrollees (Determine 6). In CY 2019, per enrollee spending for nonelderly adults who had been eligible for Medicaid on the premise of incapacity was over 5 occasions larger ($19,520) than that of youngsters and nonelderly adults who had been eligible on a non-disability foundation ($3,247). Greater spending was attributable to elevated spending on FFS LTSS and better premiums for managed care.
For many Medicaid enrollees 65 or older and plenty of enrollees with disabilities, Medicare additionally gives medical insurance. For these Medicare-Medicaid enrollees, Medicare is the first payer for a lot of medical providers together with hospitalizations, doctor visits, pharmaceuticals, preventive providers, expert nursing care, residence well being care, and hospice care. Medicaid gives protection of Medicare premiums, value sharing, and advantages that aren’t included within the Medicare program. Excessive Medicaid spending amongst Medicare-Medicaid enrollees—who’ve one other type of medical insurance—typically displays substantial LTSS spending amongst this inhabitants.
7. States should present institutional care and residential well being, however most home- and community-based providers are non-compulsory.
Medicaid LTSS spending is shifting towards HCBS settings, however most main HCBS are non-compulsory for states to cowl below Medicaid. The required HCBS are residence well being providers (outlined as part-time or intermittent nursing providers); residence well being aide providers; and medical provides, gear, and home equipment appropriate to be used within the residence. In 2020, about 734,500 individuals acquired necessary residence well being providers and these providers accounted for about 4.4% of Medicaid HCBS spending. Almost 2 million individuals used different non-compulsory state plan providers and almost three million individuals used providers via non-compulsory waiver packages (Determine 7). The variety of HCBS customers proven in Determine 7 is decrease than the variety of customers reported by the Facilities for Medicare & Medicaid Companies (CMS), which discovered that round 8 million Medicaid beneficiaries used HCBS in 2019, together with 2.3 million individuals who used residence well being. The rationale CMS knowledge present larger numbers of customers is that these knowledge outline anybody with a number of claims for a given service as an HCBS consumer, whereas the info in Determine 7 seize the inhabitants who use HCBS on an ongoing foundation.
Non-compulsory Medicaid HCBS embody private care to assist with bathing or making ready meals, therapies to assist individuals regain or purchase self-care and impartial dwelling expertise, and assistive expertise. They might be offered via state plan profit packages however are extra generally offered via HCBS waivers. HCBS waivers enable states to broaden monetary eligibility for HCBS and provide HCBS advantages focused to particular populations, resembling individuals with mental or developmental disabilities (I/DD) or individuals with bodily disabilities. In contrast to state plan advantages, HCBS waivers enable states to restrict the variety of individuals served and to waive different guidelines governing the availability of institutional care and different sorts of well being care. Many states use waivers to limit the variety of individuals utilizing HCBS and use waitlists when the variety of individuals in search of providers exceeds the variety of waiver slots out there.
8. Inside the largest class of Medicaid HCBS spending, individuals with mental and developmental disabilities accounted for over two-thirds of spending.
Almost all states provide part 1915(c) waivers, which permit states to offer LTSS in neighborhood settings as a substitute of services. In FY 2020, such waivers accounted for 51% of all Medicaid HCBS spending or about $59 billion out of about $116 billion. Throughout 47 states, 1.9 million individuals had been enrolled in 255 Medicaid 1915(c) HCBS waivers. Most of these waivers present providers to a selected inhabitants, resembling individuals over age 65, individuals with bodily disabilities, individuals with psychological disabilities, or individuals with mental and developmental disabilities (I/DD). Individuals with I/DD accounted for lower than half of general Part 1915 (c) waiver enrollment however greater than two-thirds of waiver spending on account of upper per-person spending amongst individuals in such waivers (Determine 8). The vary in per-person spending throughout waivers is sort of important. In 2020, among the many six major populations focused via 1915(c) waivers, the individual prices ranged from:
- $7,554 for individuals with HIV/AIDs (4 thousand enrollees),
- $11,677 for individuals with psychological well being circumstances (24 thousand enrollees),
- $15,211 for individuals 65+ or below 65 with disabilities (853 thousand enrollees),
- $23,092 for medically fragile or technology-depending kids (16 thousand enrollees),
- $32,425 for individuals with traumatic mind or spinal twine accidents (23 thousand enrollees), to
- $47,392 for individuals with I/DD (740 thousand enrollees).
9. Workforce shortages amongst LTSS suppliers have been exacerbated by the COVID-19 pandemic.
The pandemic drastically exacerbated shortages of LTSS staff. Employment ranges in all well being care jobs dropped sharply initially of the pandemic, however for many well being care sectors, employment began to rebound as early as spring 2020. Nonetheless, employment within the LTSS sectors continued to fall properly into 2021 and for nursing services, into the start of 2022. Current evaluation on the Peterson-KFF Well being System Tracker reveals that the variety of staff dropped by 14% in nursing care services and by 9% in neighborhood elder care services between February 2020 and June 2022 (Determine 9). As of mid-July 2022, over one in 4 licensed nursing services within the U.S. reported a scarcity of nurses and/or aides and in 2021, a survey of residence care businesses reported challenges in from staffing shortages and problem recruiting new employees. Moreover, a 50-state survey of Medicaid HCBS packages discovered that Medicaid HCBS supplier infrastructure declined in the course of the pandemic, with two-thirds of responding states reporting a everlasting closure of a minimum of one supplier. In the identical survey, states reported that workforce shortages had been the pandemic’s major influence. This isn’t stunning as a result of HCBS suppliers typically report low pay and really poor working circumstances. KFF carried out focus teams with HCBS staff throughout July and August 2021 and staff reported that the psychological calls for related to caregiving had been “overwhelming” whereas the wages had been low, the hours lengthy, and the working circumstances typically fairly demanding.
10. Wanting ahead, policymakers will proceed to face the problem of offering LTSS and the necessity for LTSS will develop because the inhabitants ages.
Almost one in 5 Individuals is projected to be 65 or older by 2060 (Determine 10). Advances in assistive and medical expertise that enable individuals with disabilities to be extra impartial and to dwell longer, along with the getting old of the newborn boomers, will doubtless lead to elevated want for LTSS over the approaching a long time. An HHS report discovered that after age 65, 57% of individuals would wish assist with a minimum of two actions of each day dwelling, 56% would use paid LTSS, and 39% would use some nursing residence care. Anticipated charges of LTSS want and use are highest amongst individuals with lifetime earnings within the backside revenue quintile, who’ve the fewest sources to pay for such care.
Though the various deaths from COVID-19 illuminated critical challenges for institutional LTSS, the identical challenges additionally have an effect on HCBS; certainly, the rising demand for care and workforce shortages could also be extra critical for residence and neighborhood settings than for establishments shifting ahead. There’s a great dearth of information on individuals utilizing HCBS and a major lack of help for paid and unpaid caregivers. The American Rescue Plan included a provision to extend the federal matching price (FMAP) for spending on Medicaid HCBS by 10 proportion factors to fund a wide range of actions to broaden entry to HCBS and help direct care suppliers. Though states’ present HCBS expenditures are now not eligible for the upper FMAP, the federal authorities just lately gave states till March 31, 2025 to spend the additional federal funds that they had already acquired. Different insurance policies which have garnered current consideration embody completely growing the FMAP for HCBS, making HCBS a compulsory profit, and increasing Medicare protection for seniors who select to go residence after a hospital keep reasonably than to a talented nursing facility. It is going to be necessary to observe whether or not and the way classes from the pandemic are built-in into new insurance policies to enhance entry to and high quality of LTSS within the U.S.






{kind=link}