
At the beginning of the pandemic, Congress enacted the Households First Coronavirus Response Act (FFCRA), which included a requirement that Medicaid packages preserve individuals constantly enrolled via the tip of the month by which the COVID-19 public well being emergency (PHE) ends, in alternate for enhanced federal funding. Primarily because of the steady enrollment requirement, Medicaid enrollment has grown considerably in comparison with earlier than the pandemic and the uninsured price has dropped. However, when the PHE ends, hundreds of thousands of individuals might lose protection that might reverse latest positive factors in protection. The present PHE ends October 15; nevertheless, it’s anticipated to be prolonged at the very least till mid-January as a result of the Biden Administration didn’t present the 60-day discover they’ve promised indicating the PHE would finish.
This temporary describes 10 key factors in regards to the unwinding of the Medicaid steady enrollment requirement, highlighting knowledge and analyses that may inform the unwinding course of in addition to steerage issued by the Facilities for Medicare and Medicaid Providers (CMS) to assist states put together for the tip of the PHE.
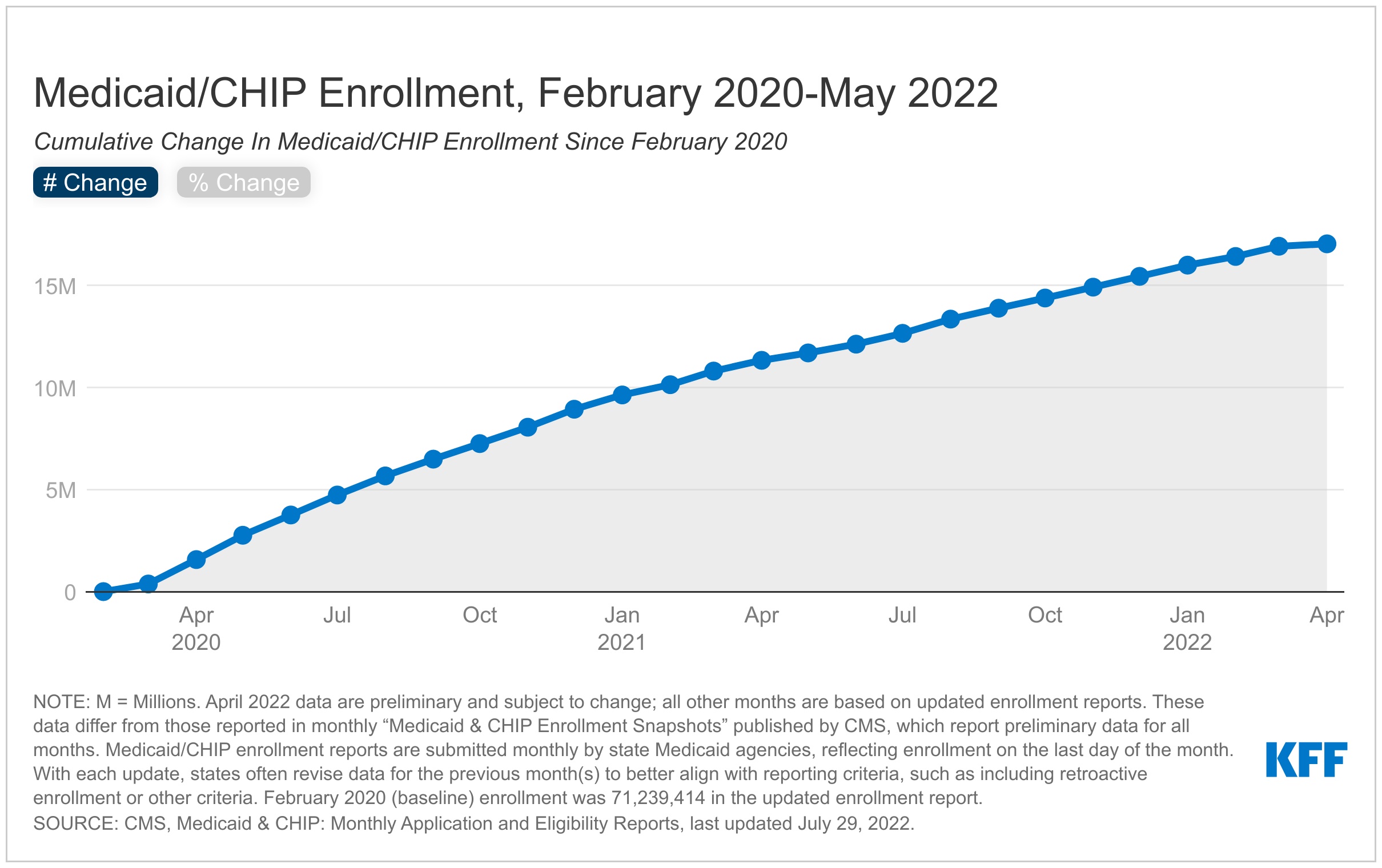
1. Medicaid enrollment has elevated for the reason that begin of the pandemic, primarily because of the steady enrollment requirement
Complete Medicaid/CHIP enrollment grew to 89.0 million in Might 2022, a rise of 17.7 million or practically 25% from enrollment in February 2020 (Determine 1). Total enrollment will increase could mirror financial circumstances associated to the pandemic, the adoption of the Medicaid growth below the Inexpensive Care Act in a number of states (NE, MO, OK), in addition to the continual enrollment requirement included within the Households First Coronavirus Response Act (FFCRA). This provision requires states to offer steady protection for Medicaid enrollees till the tip of the month by which the general public well being emergency (PHE) ends as a way to obtain enhanced federal funding. By stopping states from disenrolling individuals from protection, the continual enrollment requirement has helped to protect protection in the course of the pandemic. Nonetheless, when the PHE ends, states will start processing redeterminations and hundreds of thousands of individuals might lose protection if they’re not eligible or face administrative boundaries throughout renewals even when they proceed to be eligible. The continual protection requirement elevated state spending for Medicaid, although KFF has estimated that the improved federal funding exceeded the upper state prices.
2. KFF estimates that between 5 million and 14 million individuals will lose Medicaid protection as soon as the PHE ends.
Whereas the variety of Medicaid enrollees who could also be disenrolled in the course of the unwinding interval is extremely unsure, it’s estimated that hundreds of thousands will lose protection. Primarily based on illustrative situations—a 5% decline in complete enrollment and a 13% decline in enrollment—KFF estimates that between 5.3 million and 14.2 million individuals will lose Medicaid protection in the course of the 12-month unwinding interval (Determine 2). The decrease estimate accounts for components, reminiscent of new individuals enrolling in this system in addition to individuals disenrolling then re-enrolling in this system inside the yr, whereas the upper estimate displays complete disenrollment and doesn’t account for churn or new enrollees. These projected protection losses are in step with, although a bit decrease than, estimates from the Division of Well being and Human Providers (HHS) suggesting that as many as 15 million individuals can be disenrolled, together with 6.8 million who will possible nonetheless be eligible. Whereas the share of people disenrolled throughout states will differ attributable to variations in how states prioritize renewals, it’s anticipated that the teams that skilled probably the most progress because of the steady enrollment requirement—ACA growth adults, different adults, and kids—will expertise the most important enrollment declines. Efforts to conduct outreach, schooling and supply enrollment help might help make sure that those that stay eligible for Medicaid are capable of retain protection and those that are not eligible can transition to different sources of protection.
3. The Medicaid steady enrollment requirement has stopped “churn” amongst Medicaid enrollees.
The non permanent lack of Medicaid protection by which enrollees disenroll after which re-enroll inside a brief time period, also known as “churn,” happens for a a number of causes. Enrollees could expertise short-term adjustments in earnings or circumstances that make them quickly ineligible. Alternatively, some individuals who stay eligible could face boundaries to sustaining protection attributable to renewal processes and periodic eligibility checks. Eligible people are in danger for dropping protection if they don’t obtain or perceive notices or types requesting extra info to confirm eligibility or don’t reply to requests inside required timeframes. Churn can lead to entry boundaries in addition to extra administrative prices. Estimates point out that amongst full-benefit beneficiaries enrolled at any level in 2018, 10.3% had a niche in protection of lower than a yr (Determine 3). About 4.2% had been disenrolled after which re-enrolled inside three months and 6.9% inside six months. Nonetheless, by halting disenrollment in the course of the PHE, the continual enrollment requirement has additionally halted this churning amongst Medicaid enrollees.
4. States are required to develop plans for the way they may resume routine operations as soon as the PHE ends.
CMS requires states to develop operational plans for the way they may strategy the unwinding course of. These plans should describe how the state will prioritize renewals, how lengthy the state plans to take to finish the renewals in addition to the processes and methods the state is contemplating or has adopted to scale back inappropriate protection loss in the course of the unwinding interval. States should submit a report summarizing their plans by the forty fifth day earlier than the tip of the month by which the COVID-19 public well being emergency (PHE) ends Though CMS isn’t requiring the plans to be accredited or made publicly accessible, the company is encouraging states to interact with stakeholders in growing their plans and to make the plans public.
In accordance with a KFF survey performed in January 2022, states had been taking quite a lot of steps to organize for the tip of the PHE (Determine 4). Twenty-eight states indicated that they had settled on plan for prioritizing renewals whereas 41 stated they planning to take 12 months to finish all renewals (the remaining 10 states stated they deliberate to take lower than 12 months to finish renewals or that they had not but selected a timeframe). A majority of states additionally indicated they had been taking steps to replace enrollee contact info and had been planning to observe up with enrollees earlier than terminating protection. However the scenario is evolving–as of September 2022, 23 states had posted their full plan or a abstract of their plan publicly. How states strategy the unwinding course of can have implications for the power of eligible people to retain protection and those that are not eligible to transition to different protection. Outcomes will differ throughout states as they make completely different selections and face challenges balancing workforce capability, fiscal pressures, and the amount of labor.
5. Maximizing streamlined renewal processes can promote continuity of protection when the PHE ends.
Beneath the ACA, states should search to finish administrative (or “ex parte”) renewals by verifying ongoing eligibility via accessible knowledge sources, reminiscent of state wage databases, earlier than sending a renewal kind or requesting documentation from an enrollee. Some states suspended renewals as they carried out the MOE steady enrollment requirement and made different COVID-related changes to operations. Finishing renewals by checking digital knowledge sources to confirm ongoing eligibility reduces the burden on enrollees to keep up protection. Nonetheless, in lots of states, the share of renewals accomplished on an ex parte foundation is low. Of the 42 states processing ex parte renewals for MAGI teams (individuals whose eligibility relies on modified adjusted gross earnings), solely 11 states report finishing 50% or extra of renewals utilizing ex parte processes. Twenty-two states full lower than 50% of renewals on an ex parte foundation, together with 11 states the place lower than 25% of renewals are accomplished utilizing ex parte processes (Determine 5). The variety of states reporting they full greater than 50% of renewals utilizing ex parte processes for non-MAGI teams (individuals whose eligibility relies on being over age 65 or having a incapacity) is even decrease at 6.
As states return to routine operations when the PHE ends, there are alternatives to advertise continuity of protection amongst enrollees who stay eligible by rising the share of renewals accomplished utilizing ex parte processes and taking different steps to streamline renewal processes (which may even have a tendency to extend enrollment and spending). CMS notes in latest steerage that states can improve the share of ex parte renewals they full with out having to observe up with the enrollee by increasing the info sources they use to confirm ongoing eligibility. Nonetheless, when states do have to observe up with enrollees to acquire extra info to substantiate ongoing eligibility, they’ll facilitate receipt of that info by permitting enrollees to submit info by mail, in particular person, over the cellphone, and on-line. Whereas practically all states settle for info by mail and in particular person, barely fewer present choices for people to submit info over the cellphone (39 states) or via on-line accounts (41 states). A latest proposed rule, launched on September 7, 2022, seeks to streamline enrollment and renewal processes sooner or later by making use of the identical guidelines for MAGI and non-MAGI populations, together with limiting renewals to as soon as per yr, prohibiting in-person interviews and requiring the usage of prepopulated renewal types.
6. States can receive non permanent waivers to pursue methods to assist their unwinding plans.
As states put together to finish redeterminations for all Medicaid enrollees as soon as the PHE ends, many could face vital operational challenges associated to staffing shortages and outdated methods. To cut back the executive burden on states, CMS introduced the supply of non permanent waivers via Part 1902(e)(14)(A) of the Social Safety Act. These waivers can be accessible on a time-limited foundation and can allow states to facilitate the renewal course of for sure enrollees with the purpose minimizing procedural terminations. In steerage launched on March 3, 2022, CMS outlined 5 focused methods for these waivers that embrace: renewing enrollee protection based mostly on SNAP eligibility; permitting for ex parte renewals of people with zero earnings verified inside the previous 12 months; permitting for renewals of people whose belongings can’t be verified via the asset verification system (AVS); partnering with managed care organizations (MCOs) or utilizing the Nationwide Change of Handle (NCOA) database or US postal service (USPS) returned mail to replace enrollee contact info; and increasing the timeframe for truthful listening to requests. Nonetheless, it additionally famous that the company would take into account different renewal technique requests that influence the state’s means to course of renewals. As of September 6, 2022, CMS had accredited a complete of 84 waivers for 27 states (Determine 6).
7. Individuals who have moved for the reason that begin of the pandemic, these with restricted English proficiency (LEP) and other people with disabilities, could also be at higher threat for dropping Medicaid protection when the PHE ends.
When the continual enrollment necessities finish and states resume redeterminations and disenrollments, sure people can be at elevated threat of dropping Medicaid protection or experiencing a niche in protection attributable to boundaries finishing the renewal course of, even when they continue to be eligible for protection. Enrollees who’ve moved could not obtain essential renewal and different notices, particularly in the event that they haven’t up to date their contact info with the state Medicaid company. In 2020, one in ten Medicaid enrollees moved in-state in 2020 and whereas shares of Medicaid enrollees transferring inside a state has trended downward in recent times, these developments might have modified in 2021, as extra individuals grew to become vaccinated towards COVID-19 and the nationwide eviction moratorium was lifted in August 2021. Moreover, individuals with LEP and other people with disabilities usually tend to encounter challenges attributable to language and different boundaries accessing info in wanted codecs. A latest evaluation of state Medicaid web sites discovered that whereas a majority of states translate their on-line software touchdown web page or PDF software into different languages, most solely present Spanish translations (Determine 7). That very same evaluation revealed {that a} majority of states present common details about affordable modifications and teletypewriter (TTY) numbers on or inside one click on of their homepage or on-line software touchdown web page (Determine 8), however fewer states present info on how you can entry functions in massive print or Braille or how you can entry American Signal Language interpreters.
CMS steerage in regards to the PHE unwinding stresses the significance of conducting outreach to enrollees to replace contact info and gives methods for partnering with different organizations to extend the chance that enrollee addresses and cellphone numbers are updated. CMS steerage additionally outlines particular steps states can take, together with making certain accessibility of types and notices for individuals with LEP and other people with disabilities and reviewing communications methods to make sure accessibility of data. Making certain accessibility of data, types, and help can be key for stopping protection losses and gaps amongst these people.
8. States can accomplice with MCOs, neighborhood well being facilities, and different trusted companions to conduct outreach.
As the tip of the PHE approaches, states can collaborate with well being plans and neighborhood organizations to conduct outreach to enrollees to organize them for the tip of the continual enrollment requirement. CMS has issued particular steerage permitting states to allow MCOs to replace enrollee contact info and facilitate continued enrollment; nevertheless, states may also work with neighborhood well being facilities, navigators and different assister packages, and community-based organizations to offer info to enrollees and help them with updating contact info earlier than the PHE ends, finishing the Medicaid renewal course of as soon as the PHE ends, and transitioning to different protection if they’re not eligible. In accordance with a latest survey of Medicaid packages, 39 states indicated they plan to work with different state companies and stakeholders, together with 32 that plan to accomplice with MCOs, to help non-MAGI Medicaid enrollees when the PHE ends. An analogous survey performed earlier within the yr discovered that 25 states stated they had been planning to request MCOs to contact MAGI Medicaid enrollees to replace mailing addresses.
States can make the most of actions potential companions are already taking or planning to take to organize for the unwinding. A survey of well being facilities performed in late 2021 discovered that just about 50% of responding well being facilities reported they’ve or plan to succeed in out to their Medicaid sufferers with reminders to resume their protection and to schedule appointments to help them with renewing protection (Determine 9).
9. Well timed knowledge on disenrollments and different metrics can be helpful for monitoring how the unwinding is continuing.
In March, CMS introduced new knowledge necessities for states to gather and report knowledge on eligibility and enrollment metrics previous to and in the course of the unwinding interval in addition to their plans for initiating and finishing renewals in the course of the unwinding interval. Particularly, CMS directs states to submit an preliminary baseline report that captures eligibility and enrollment knowledge within the month previous to the tip of the PHE. The baseline report consists of 4 knowledge metrics—pending functions, complete enrollment, estimated timeframe for finishing initiated renewals, and truthful hearings pending for greater than 90 days (Determine 10). As soon as the PHE ends, states can be required to submit month-to-month studies that seize each cumulative and noncumulative knowledge on software processing, renewals initiated and the outcomes of the renewals, and pending Medicaid truthful hearings in the course of the unwinding interval. CMS has not dedicated to creating these knowledge public, probably limiting their utility for broader monitoring; nevertheless, some states have indicated they plan to create knowledge dashboards or make key unwinding knowledge publicly accessible.
These metrics are designed to display states’ progress in the direction of restoring well timed software processing and initiating and finishing renewals of eligibility for all Medicaid and CHIP enrollees and may help with monitoring the unwinding course of to determine issues as they happen. Nonetheless, whereas the brand new knowledge reporting necessities are helpful, they won’t present an entire image of how the unwinding is continuing and whether or not sure teams face boundaries to sustaining protection. To totally assess the influence of the unwinding would require broader end result measures, reminiscent of continuity of protection throughout Medicaid, CHIP, Market, and employer protection, gaps in protection over time, and will increase within the variety of the uninsured, knowledge that won’t be accessible within the short-term.
10. The variety of individuals with out medical insurance might improve if individuals who lose Medicaid protection are unable to transition to different protection.
The share of people that lack medical insurance protection dropped to eight.6% in 2021, matching the historic low in 2016, largely due to will increase in Medicaid protection, and to a lesser extent, will increase in Market protection. Nonetheless, when states resume Medicaid disenrollments on the finish of the PHE, these protection positive factors could possibly be reversed. CMS steerage gives a roadmap for states to streamline processes and implement different methods to scale back the quantity of people that lose protection regardless that they continue to be eligible. Nonetheless, there may even be present enrollees who’re decided to be not be eligible for Medicaid, however who could also be eligible for ACA market or different protection. A latest MACPAC evaluation examined protection transitions for adults and kids who had been disenrolled from Medicaid or separate CHIP (S-CHIP) and located that only a few adults or kids transitioned to federal Market protection, solely 21% of kids transitioned from Medicaid to S-CHIP, whereas 47% of kids transitioned from S-CHIP to Medicaid (Determine 11). These findings recommend that people face boundaries transferring from Medicaid to different protection packages, together with S-CHIP. Simplifying these transitions to scale back the boundaries individuals face might assist guarantee people who find themselves not eligible for Medicaid don’t change into uninsured. The latest proposed rule goals to easy transitions between Medicaid and CHIP by requiring the packages to simply accept eligibility determinations from the opposite program, to develop procedures for electronically transferring account info, and to offer mixed notices.





{kind=link}