
The Inflation Discount Act of 2022, signed into legislation by President Biden on August 16, 2022, consists of a number of provisions to decrease prescription drug prices for individuals with Medicare and cut back drug spending by the federal authorities. This laws has taken form amidst robust bipartisan, public help for the federal government to handle excessive and rising drug costs. CBO estimates that the drug pricing provisions within the reconciliation invoice will cut back the federal deficit by $237 billion over 10 years (2022-2031).
The prescription drug proposals included within the Inflation Discount Act will:
This transient summarizes these provisions and discusses the anticipated results on individuals, program spending, and drug costs and innovation.
Require the Federal Authorities to Negotiate Costs for Some Medicine Lined Beneath Medicare
Beneath the Medicare Half D program, which covers retail pharmaceuticals, Medicare contracts with personal plan sponsors to supply a prescription drug profit. The legislation that established the Half D profit included a provision often known as the “noninterference” clause, which stipulates that the HHS Secretary “might not intervene with the negotiations between drug producers and pharmacies and PDP [prescription drug plan] sponsors, and should not require a selected formulary or institute a worth construction for the reimbursement of coated half D medicine.” As well as, the Secretary of HHS doesn’t at the moment negotiate costs for medicine coated beneath Medicare Half B (administered by physicians). As a substitute, Medicare reimburses suppliers primarily based on a formulation set at 106% of the Common Gross sales Worth (ASP), which is the typical worth to all non-federal purchasers within the U.S, inclusive of rebates (apart from rebates paid beneath the Medicaid program).
The Half D non-interference clause has been a longstanding goal for some policymakers as a result of it has restricted the power of the federal authorities to leverage decrease costs, significantly for high-priced medicine with out opponents. Medicare Half D and Half B drug spending is extremely concentrated amongst a comparatively small share of coated medicine, primarily these with out generic or biosimilar opponents. A current KFF Monitoring Ballot finds massive majorities help permitting the federal authorities to barter drug costs and this help holds regular even after the general public is supplied with the arguments that have been made for and towards this proposal.
Provision Description
The Inflation Discount Act amends the non-interference clause by including an exception that requires the Secretary of HHS to barter costs with drug corporations for a small variety of single-source brand-name medicine or biologics with out generic or biosimilar opponents which can be coated beneath Medicare Half D (beginning in 2026) and Half B (beginning in 2028). Beneath the brand new Drug Worth Negotiation Program, the variety of medicine topic to cost negotiation will likely be 10 Half D medicine for 2026, one other 15 Half D medicine for 2027, one other 15 Half D and Half B medicine for 2028, and one other 20 Half D and Half B medicine for 2029 and later years. These medicine will likely be chosen from among the many 50 medicine with the very best complete Medicare Half D spending and the 50 medicine with the very best complete Medicare Half B spending. The variety of medicine with negotiated costs obtainable will accumulate over time.
Sure classes of medicine are excluded from the negotiation course of, together with:
- Medicine which have a generic or biosimilar obtainable
- Medicine which can be lower than 9 years (for small-molecule medicine) or 13 years (for organic merchandise) from their FDA-approval or licensure date
- “Small biotech medicine” (till 2029), outlined as these which account for 1% or much less of Half D or Half B spending and account for 80% or extra of spending beneath every half on that producer’s medicine
- Medicine with Medicare spending of lower than $200 million in 2021 (elevated by the CPI-U for subsequent years)
- Medicine with an orphan designation as their solely FDA-approved indication
- All plasma-derived merchandise
The laws additionally delays number of biologic medicine for negotiation by as much as two years if a biosimilar product is more likely to enter the market in that point.
The legislation establishes an higher restrict for the negotiated worth (the “most honest worth”) for a given drug. The restrict is the decrease of the drug’s enrollment-weighted negotiated worth (web of all worth concessions) for a Half D drug, the typical gross sales worth for a Half B drug, or a proportion of a drug’s common non-federal common producer worth: 75% for small-molecule medicine and vaccines greater than 9 years however lower than 12 years past approval; 65% for medicine between 12 and 16 years past approval or licensure; and 40% for medicine greater than 16 years past approval or licensure.
Half D medicine with negotiated “most honest costs” are required to be coated by all Half D plans. Medicare’s fee to suppliers for Half B medicine with negotiated costs will likely be 106% of the utmost honest worth (somewhat than the present fee of 106% of the typical gross sales worth). (A separate part of the legislation will increase Medicare funds to suppliers for the administration of biosimilar biologic merchandise to 108% of the typical gross sales worth from October 1, 2022 via December 31, 2027.)
An excise tax will likely be levied on drug corporations that don’t adjust to the negotiation course of. The excise tax begins at 65% of a product’s gross sales within the U.S. and will increase by 10% each quarter to a most of 95%. As a substitute for paying the tax, producers can select to withdraw all of their medicine from protection beneath Medicare and Medicaid. As well as, producers that refuse to supply an agreed-upon negotiated worth for a particular drug to “a most honest worth eligible particular person” (i.e., Medicare beneficiaries enrolled in Half B and/or Half D) or to a supplier of companies to most honest worth eligible people (akin to a doctor or hospital) pays a civil financial penalty equal to 10 occasions the distinction between the worth charged and the utmost honest worth.
The timeline for the negotiation course of spans roughly two years, though the timeline is modified for 2026, the primary 12 months that negotiated costs will likely be obtainable beneath this new program (Determine 1). For the ten Half D medicine with negotiated costs taking impact on January 1, 2026, the record of 10 Half D medicine chosen for negotiation will likely be printed on September 1, 2023, primarily based on spending knowledge for the 12-month interval from June 1, 2022 to Could 31, 2023. The interval of negotiation between the Secretary and producers of those medicine will happen between October 1, 2023 and August 1, 2024, and the negotiated “most honest costs” will likely be printed no later than September 1, 2024. For 2027, which is an instance of timing for a typical 12 months by way of the timeline for establishing negotiated costs, the record of 15 Half D medicine chosen for negotiation will likely be printed on February 1, 2025. The interval of negotiation between the Secretary and producers of the chosen medicine will happen between February 28, 2025 and November 1, 2025 and the negotiated “most honest costs” will likely be printed no later than November 30, 2025. For Half B medicine, the preliminary interval of drug worth negotiation between the Secretary and producers of chosen medicine will happen between February 28, 2026 and November 1, 2026, with negotiated costs first obtainable in 2028.
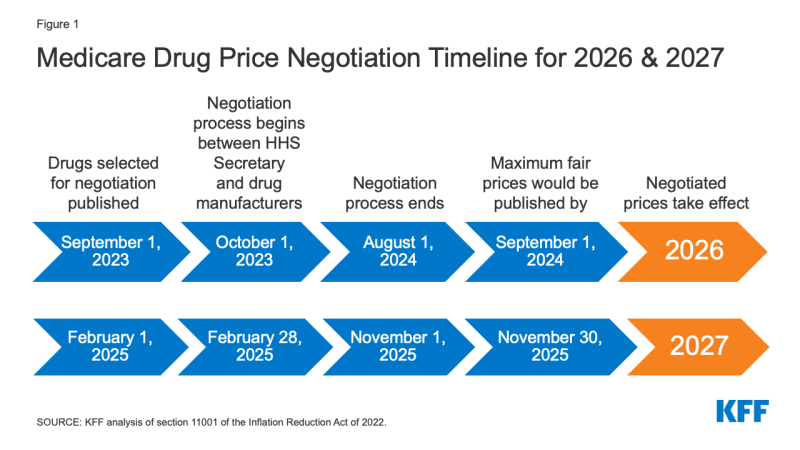
Determine 1: Medicare Drug Worth Negotiation Timeline for 2026 & 2027
The laws appropriates funding of $3 billion in fiscal 12 months 2022 for implementing the drug worth negotiation provisions over the 2023-2031 interval.
Efficient Date
Negotiated costs for the primary set of chosen medicine coated beneath Half D will likely be obtainable in 2026. For medicine coated beneath Half B, the primary 12 months negotiated costs will likely be obtainable is 2028.
Individuals affected
The supply to permit the Secretary to barter drug costs will put downward stress on each Half D premiums and out-of-pocket drug prices, though the variety of Medicare beneficiaries who will see decrease out-of-pocket drug prices in any given 12 months beneath the drug worth negotiation program and the magnitude of financial savings will rely on what number of and which medicine are topic to the negotiation course of and the worth reductions achieved via the negotiations course of relative to what costs would in any other case be.
budgetary affect
CBO estimates $98.5 billion in Medicare financial savings over 10 years (2022-2031) from the drug negotiation provisions within the Inflation Discount Act.
Results on the Growth of New Medicine
CBO estimates that the drug pricing provisions within the Inflation Discount Act, together with however not restricted to the brand new Medicare drug worth negotiation program, could have a really modest affect on the variety of new medicine coming to market within the U.S. over the following 30 years: 13 fewer out of 1,300, or a discount of 1% (about 1 fewer drug over the 2023-2032 interval, about 5 fewer medicine within the subsequent decade, and about 7 fewer medicine within the decade after that).
Require Drug Producers to Pay Rebates for Worth Will increase Above Inflation for Medicine Utilized by Individuals with Medicare
Thus far, Medicare has had no authority to restrict annual worth will increase for medicine coated beneath Half B or Half D. In distinction, Medicaid has a rebate system that requires drug producers to supply refunds if costs develop quicker than inflation. Yr-to-year drug worth will increase exceeding inflation should not unusual and have an effect on individuals with each Medicare and personal insurance coverage. Our evaluation reveals that half of all medicine coated by Medicare had record worth will increase that exceeded the speed of inflation between 2019 and 2020. A separate evaluation by the HHS Workplace of Inspector Basic confirmed common gross sales worth (ASP) will increase exceeding inflation for 50 of 64 studied Half B medicine in 2015.
provision description
The Inflation Discount Act requires drug producers to pay a rebate to the federal authorities if costs for single-source medicine and biologicals coated beneath Medicare Half B and practically all coated medicine beneath Half D enhance quicker than the speed of inflation (CPI-U). Worth modifications will likely be measured primarily based on the typical gross sales worth for Half B medicine and the typical producer worth for Half D medicine. If worth will increase are larger than inflation, producers will likely be required to pay the distinction within the type of a rebate to Medicare. The rebate quantity is the same as the entire variety of items bought in Medicare multiplied by the quantity, if any, by which a drug’s worth in a given 12 months exceeds the inflation-adjusted worth. The bottom 12 months for measuring cumulative worth modifications relative to inflation is 2021.
Rebate {dollars} could be deposited within the Medicare Supplementary Medical Insurance coverage (SMI) belief fund. Producers that don’t pay the required rebate quantity will face a penalty equal to no less than 125% of the unique rebate quantity.
The laws appropriates 10-year (2022-2031) funding of $160 million to the Facilities for Medicare & Medicaid Companies (CMS) for implementing the inflation rebate provisions ($80 million for Half B and $80 million for Half D).
Efficient Date
The Half D inflation rebate provision takes impact in 2022, the place to begin for measuring drug worth will increase, with rebate funds required starting in 2023. The Half B inflation rebate provision takes impact in 2023.
Individuals affected
These provisions are anticipated to restrict out-of-pocket drug spending development for individuals with Medicare and put downward stress on premiums by discouraging drug corporations from rising costs quicker than inflation. The variety of Medicare beneficiaries who will see decrease out-of-pocket drug prices in any given 12 months ensuing from these provisions will rely on what number of and which medicine have lower cost will increase and the magnitude of worth reductions relative to what costs would in any other case be.
budgetary affect
CBO estimates a web federal deficit discount of $63.2 billion over 10 years (2022-2031) from the drug inflation rebate provisions within the Inflation Discount Act. This consists of web financial savings of $56.3 billion ($71.8 billion in financial savings to Medicare and $0.3 billion in financial savings for different federal applications, akin to DoD, FEHB, and subsides for ACA Market protection, offset by $15.7 billion in further Medicaid spending) and better federal revenues of $6.9 billion.
Results on Launch Pricing
Drug producers might reply to the inflation rebates by rising launch costs for medicine that come to market sooner or later. CBO tasks that larger launch costs would primarily have an effect on Medicaid spending. It’s because, though the essential Medicaid drug rebate could be bigger (since it’s calculated as a proportion of the typical producer worth), the upper Medicaid drug rebates wouldn’t offset larger launch costs. In response to CBO, Medicare Half D plan sponsors and personal insurers could be much less affected than Medicaid by larger launch costs as a result of they might nonetheless be capable to negotiate rebates with drug corporations and probably refuse to cowl medicine with very excessive launch costs. Nevertheless, they might have much less leverage in some cases, akin to when there aren’t any therapeutic options obtainable or when medicine are coated beneath a Half D “protected class”. As well as, if launch costs rise for Half B medicine, the HHS Secretary would don’t have any authority to barter decrease costs except and till the brand new drug meets the factors for choice for drug worth negotiation beneath the negotiation course of described above.
Cap Out-of-Pocket Spending for Medicare Half D Enrollees and Different Half D Profit Design Adjustments
Medicare Half D at the moment offers catastrophic protection for prime out-of-pocket drug prices, however there is no such thing as a restrict on the entire quantity that beneficiaries pay out of pocket annually. Beneath the present profit design, Half D enrollees qualify for catastrophic protection when the quantity that they pay out of pocket plus the worth of the producer low cost on the worth of brand-name medicine within the protection hole part exceeds a sure threshold quantity. Enrollees with drug prices excessive sufficient to exceed the catastrophic threshold are required to pay 5% of their complete drug prices above the brink till the top of the 12 months except they qualify for Half D Low-Revenue Subsidies (LIS). In 2022, the catastrophic threshold is ready at $7,050, and beneficiaries pay about $3,000 out of pocket for brand-name medicine earlier than reaching the catastrophic protection part.
Medicare pays 80% of complete prices above the catastrophic threshold (often known as “reinsurance”) and plans pay 15%. Medicare’s reinsurance funds to Half D plans now account for near half of complete Half D spending (47%), up from 14% in 2006 (rising from $6 billion in 2006 to $52 billion in 2021).
Beneath the present construction of Half D, there are a number of phases, together with a deductible, an preliminary protection part, a protection hole part, and the catastrophic part. In the course of the protection hole profit part, enrollees pay 25% of drug prices for each brand-name and generic medicine; plan sponsors pay 5% for manufacturers and 75% for generics; and drug producers present a 70% worth low cost on manufacturers (there is no such thing as a low cost on generics). Beneath the present profit design, beneficiaries can face totally different cost-sharing quantities for a similar treatment relying on which part of the profit they’re in, and may face vital out-of-pocket prices for high-priced medicine due to coinsurance necessities and no exhausting out-of-pocket cap.
provision description
The Inflation Discount Act amends the design of the Half D profit. For 2024, the legislation eliminates the 5% beneficiary coinsurance requirement above the catastrophic protection threshold, successfully capping out-of-pocket prices at roughly $3,250 that 12 months. Starting in 2025, the laws provides a tough cap on out-of-pocket spending of $2,000, listed in future years to the speed of enhance in per capita Half D prices (Determine 2).
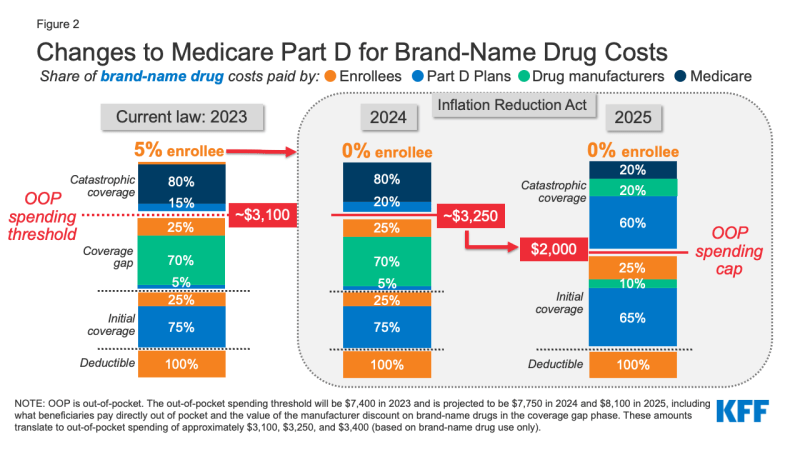
Determine 2: Adjustments to Medicare Half D for Model-Identify Drug Prices
The legislation additionally modifies legal responsibility for Medicare Half D plans and drug producers, beginning in 2025, and reduces Medicare’s legal responsibility for spending above the out-of-pocket cap. Medicare’s share of complete prices above the spending cap (“reinsurance”) will lower from 80% to twenty% for brand-name medicine and to 40% for generic medicine. Medicare Half D plans’ share of prices will enhance from 15% to 60% for each manufacturers and generics above the cap, and drug producers will likely be required to supply a 20% worth low cost on brand-name medicine. The laws additionally requires producers to supply a ten% low cost on brand-name medicine between the deductible and the annual out-of-pocket spending cap, changing the 70% worth low cost within the protection hole part beneath the present profit design.
The legislation additionally offers for an adjustment to the calculation of the bottom beneficiary premium for 2024 via 2029, limiting premium will increase to not more than 6% from the prior 12 months. For 2030, the invoice features a provision to decrease the beneficiary share of the price of commonplace drug protection (at the moment set at 25.5%) to make sure that the premium doesn’t enhance by greater than 6% from 2029. The laws additionally permits Half D enrollees the choice of spreading out their out-of-pocket prices over the 12 months somewhat than face excessive out-of-pocket prices in any given month.
Efficient Date
The Half D profit redesign provisions take impact starting in 2024, with the elimination of the 5% coinsurance for catastrophic protection and the primary 12 months of the Half D premium adjustment. Different modifications take impact in 2025, together with the $2,000 cap on out-of-pocket drug spending, spreading out of prices, and modifications to legal responsibility for complete prices above the spending cap.
individuals affected
Medicare beneficiaries in Half D plans with comparatively excessive out-of-pocket drug prices are more likely to see substantial out-of-pocket value financial savings from these modifications. This consists of Medicare beneficiaries with spending above the catastrophic threshold because of only one very high-priced specialty drug for medical situations akin to most cancers, hepatitis C, or a number of sclerosis and beneficiaries who take a handful of comparatively pricey model or specialty drugs to handle their medical situations.
Based mostly on our evaluation, 1.4 million Half D enrollees incurred annual out-of-pocket prices for his or her drugs above $2,000 in 2020, averaging $3,355 per particular person. This estimate consists of 1.3 million enrollees who had spending above the catastrophic protection threshold (which equaled roughly $2,700 in out-of-pocket prices that 12 months for brand-name medicine alone). These estimates are a conservative measure of what number of beneficiaries will likely be helped by capping out-of-pocket drug spending beneath Medicare Half D beginning in 2024 as a result of they don’t account for anticipated will increase in annual out-of-pocket drug spending between 2020 and 2024/2025, the rise within the variety of beneficiaries on Medicare, or larger utilization and spending related to the elevated affordability of pharmaceuticals because of this profit enchancment.
Based mostly on their common out-of-pocket spending, these 1.4 million Half D enrollees would have saved $1,355, or 40% of their annual out-of-pocket prices, on common, if a $2,000 cap had been in place in 2020. Half D enrollees with higher-than-average out-of-pocket prices will save substantial quantities with a $2,000 out-of-pocket spending cap. For instance, the highest 10% of beneficiaries (145,000 enrollees) with common out-of-pocket prices for his or her drugs above $2,000 in 2020 – who spent no less than $5,567 – would have saved $3,567 (64%) in out-of-pocket prices with a $2,000 cap.
Capping out-of-pocket drug spending beneath Medicare Half D will likely be particularly useful for beneficiaries who take high-priced medicine for situations akin to most cancers or a number of sclerosis. For instance, in 2020, amongst Half D enrollees with out low-income subsidies, common annual out-of-pocket spending for the most cancers drug Revlimid was $6,200 (utilized by 33,000 beneficiaries); $5,700 for the most cancers drug Imbruvica (utilized by 21,000 beneficiaries); and $4,100 for the MS drug Avonex (utilized by 2,000 beneficiaries).
With the brand new exhausting cap on out-of-pocket spending, it’s attainable that enrollees may face larger Half D premiums ensuing from larger plan legal responsibility for drug prices above the spending cap, although these premium will increase may very well be mitigated by the provisions to stabilize premiums between 2024 and 2030. Plans will probably face monetary incentives to train higher management of prices under the brand new spending cap, akin to via extra utilization administration or elevated generic drug utilization, which may assist to restrict potential premium will increase.
budgetary affect
CBO estimates these provisions will enhance federal spending by $30 billion over 10 years (2022-2031), which consists of $29.9 billion in larger spending related to Half D profit redesign and $0.1 billion in larger spending related to the supply to unfold out out-of-pocket prices.
Restrict Price Sharing for Insulin for Individuals with Medicare
For Medicare beneficiaries with diabetes who use insulin, protection is offered beneath Medicare Half D, the outpatient prescription drug profit, and can also be coated beneath Half B when used with an exterior insulin pump. As a result of Half D plans range by way of the insulin merchandise they cowl and prices per prescription, what enrollees pay for insulin merchandise additionally varies. Beneficiary coinsurance beneath Medicare Half B is 20% of the Medicare-approved quantity.
At present, Medicare beneficiaries can select to enroll in a Half D plan taking part in an Innovation Middle mannequin wherein enhanced drug plans cowl insulin merchandise at a month-to-month copayment of $35 within the deductible, preliminary protection, and protection hole phases of the Half D profit. Collaborating plans do not need to cowl all insulin merchandise on the $35 month-to-month copayment quantity, simply one among every dosage kind (vial, pen) and insulin kind (rapid-acting, short-acting, intermediate-acting, and long-acting). In 2022, a complete of two,159 Half D plans are taking part on this mannequin, or roughly one third of all Half D plans. Practically half (45%) of non-LIS enrollees are in PDPs taking part within the insulin mannequin in 2022, primarily based on August 2021 enrollment. The mannequin was launched in response to rising costs for insulin, which have attracted rising scrutiny from policymakers, resulting in congressional investigations and total considerations about affordability and entry for individuals with diabetes who want insulin to regulate blood glucose ranges.
provision description
The Inflation Discount Act limits month-to-month value sharing for insulin merchandise to not more than $35 for Medicare beneficiaries, together with insulin coated beneath each Half D and Half B, and no deductible will apply. All Medicare Half D plans, each stand-alone drug plans and Medicare Benefit drug plans, will likely be required to cost not more than $35 for whichever insulin merchandise they cowl, though plans won’t be required to cowl all insulin merchandise. For 2026 and past, the legislation limits month-to-month Half D copayments for insulin to the lesser of $35, 25% of the utmost honest worth (in circumstances the place the insulin product has been chosen for negotiation), or 25% of the negotiated worth in Half D plans.
Efficient Date
The month-to-month cap on insulin value sharing in Medicare takes impact in 2023.
Individuals affected
A $35 cap on month-to-month value sharing for insulin merchandise is predicted to decrease out-of-pocket prices for insulin customers in Medicare Half D with out low-income subsidies. In 2020, 3.3 million Medicare Half D enrollees used insulin. Amongst Medicare Half D insulin customers who don’t obtain low-income subsidies, common out-of-pocket prices per prescription throughout all insulin merchandise was $54 in 2020 – over 50% greater than the $35 month-to-month copay cap for insulin that can start in 2023.
In response to our evaluation of 2019 Half D formularies, numerous Half D plans positioned insulin merchandise on Tier 3, the popular drug tier, which usually had a $47 copayment per prescription through the preliminary protection part. Nevertheless, as soon as enrollees reached the protection hole part, they confronted a 25% coinsurance fee, which equates to $100 or extra per prescription in out-of-pocket prices for a lot of insulin therapies, except they certified for low-income subsidies. Paying a flat $35 copayment somewhat than 25% coinsurance or a better copayment quantity may cut back out-of-pocket prices for a lot of insulin merchandise.
budgetary affect
CBO estimates further federal spending of $5.1 billion ($4.8 billion for Medicare Half D and $0.3 billion for Medicare Half B) over 10 years (2022-2031) related to the insulin cost-sharing limits within the Inflation Discount Act.
Eradicate Price Sharing for Grownup Vaccines Lined Beneath Half D and Enhance Entry to Grownup Vaccines in Medicaid and CHIP
Medicare covers vaccines beneath each Half B and Half D. This separation of protection for vaccines beneath Medicare is as a result of there have been statutory necessities for protection of a small variety of vaccines beneath Half B earlier than the 2006 begin of the Half D profit. Vaccines for COVID-19, influenza, pneumococcal illness, and hepatitis B (for sufferers at excessive or intermediate danger), and vaccines wanted to deal with an harm or publicity to illness are coated beneath Half B. All different commercially obtainable vaccines wanted to forestall sickness are coated beneath Medicare Half D.
For the influenza, pneumococcal pneumonia, hepatitis B, and COVID-19 vaccines coated beneath Medicare Half B, sufferers at the moment face no value sharing for both the vaccine itself or its administration. For different Half B vaccines, akin to these wanted to deal with an harm or publicity to a illness akin to rabies or tetanus, Medicare covers 80% of the associated fee, and beneficiaries are chargeable for the remaining 20%. In contrast to most vaccines coated beneath Half B, vaccines coated beneath Half D might be topic to value sharing, as a result of Half D plans have flexibility to find out how a lot enrollees will likely be required to pay for any given on-formulary drug, together with vaccines. (Half D enrollees who obtain low-income subsidies (LIS) typically pay comparatively low quantities for vaccines and different coated medicine.) Beneath Half D, value sharing can take the type of flat greenback copayments or coinsurance (i.e., a proportion of record worth).
With regard to Medicaid and CHIP, protection of grownup vaccines is non-compulsory and varies by state. In response to a current survey, half of states (25) didn’t cowl all vaccines beneficial by the Advisory Committee on Immunization Practices (ACIP) in 2018–2019, and 15 of 44 states responding to the survey imposed value sharing necessities on grownup vaccines.
provision description
The Inflation Discount Act requires that grownup vaccines coated beneath Medicare Half D which can be beneficial by the Advisory Committee on Immunization Practices (ACIP), akin to for shingles, be coated for free of charge. This makes protection of vaccines beneath Medicare Half D per protection of vaccines beneath Medicare Half B, such because the flu and COVID-19 vaccines. The legislation additionally requires state Medicaid and CHIP applications to cowl all accredited grownup vaccines beneficial by ACIP and vaccine administration, with out value sharing.
Efficient Date
These provisions take impact in 2023.
Individuals affected
Eliminating cost-sharing for grownup vaccines coated beneath Medicare Half D may assist with vaccine uptake amongst older adults and can decrease out-of-pocket prices for many who want Half D-covered vaccines. Our evaluation reveals that in 2020, 4.1 million Medicare beneficiaries acquired a Half D-covered vaccine, together with 3.6 million who acquired the vaccine to forestall shingles, and combination out-of-pocket spending on Half D vaccines was $0.3 billion. In 2018, Half D enrollees with out low-income subsidies paid a median of $57 out of pocket for every dose of the shingles shot, which is mostly free to most different individuals with personal protection.
Requiring state Medicaid and CHIP applications to cowl all grownup vaccines beneficial by ACIP with out value sharing is predicted to extend entry to some grownup vaccines beneath Medicaid. Utilizing a current survey’s state degree knowledge and 2019 grownup Medicaid enrollment knowledge, a separate KFF evaluation estimates about 4 million adults may acquire protection of no less than a number of vaccines.
budgetary affect
CBO estimates that these provisions will enhance federal spending by $7 billion over 10 years (2022-2031), together with $4.4 billion for Medicare and $2.5 billion for Medicaid and CHIP.
Develop Eligibility for Half D Low-Revenue Subsidies
provision description
The Half D Low-Revenue Subsidy (LIS) Program helps beneficiaries with their Half D premiums, deductibles, and price sharing, offering various ranges of help to beneficiaries at totally different earnings and asset ranges as much as 150% of poverty. Based mostly on knowledge from CMS, in 2020, 13.1 million Medicare beneficiaries acquired both full or partial LIS advantages, representing 28% of all Half D enrollees that 12 months.
Medicare beneficiaries who’re additionally enrolled in Medicaid, who typically have incomes as much as 135% of poverty, routinely obtain full LIS advantages. People who don’t routinely qualify for LIS can enroll in the event that they meet sure earnings and asset necessities set by the federal authorities and may obtain full or partial LIS advantages relying on their earnings and belongings. Beneficiaries qualify for full LIS advantages if they’ve earnings as much as 135% of poverty and assets as much as $9,900 particular person, $15,600 couple in 2022 (together with a $1,500 per particular person allowance for funeral/burial bills). Beneficiaries qualify for partial LIS advantages if they’ve earnings between 135-150% of poverty and assets as much as $15,510 particular person, $30,950 couple in 2022.
Beneficiaries who obtain full LIS advantages pay no Half D premium or deductible and solely modest copayments for pharmaceuticals till they attain the catastrophic threshold, at which level they face no further value sharing. Some beneficiaries who obtain partial LIS advantages pay no month-to-month premium whereas others pay a partial month-to-month Half D premium (with subsidies of 75%, 50%, or 25% of the month-to-month premium, relying on their earnings); all partial LIS recipients additionally pay an $89 annual deductible (in 2022), 15% coinsurance as much as the out-of-pocket threshold, and modest copayments for medicine above the catastrophic threshold.
The Inflation Discount Act makes people with incomes as much as 150% of poverty and assets at or under the boundaries for partial LIS advantages eligible for full advantages beneath the Half D Low-Revenue Subsidy Program. The legislation eliminates the partial LIS profit at the moment in place for people with incomes between 135% and 150% of poverty.
Efficient Date
Growth of eligibility for full Half D LIS advantages takes impact in 2024.
Individuals affected
Offering full Medicare Half D LIS advantages to Half D enrollees with incomes as much as 150% of poverty may assist an estimated 0.4 million beneficiaries, primarily based on the variety of beneficiaries receiving partial LIS advantages in 2020. Annual out-of-pocket drug prices for these beneficiaries may fall by near $300, on common, primarily based on the distinction between common out-of-pocket drug prices for LIS enrollees receiving full advantages versus partial advantages in 2020 – plus further financial savings related to extra beneficiant premium subsidies.
These averages understate the potential value financial savings for the smaller share of low-income enrollees with terribly excessive drug prices, akin to partial LIS beneficiaries who take high-cost specialty medicine. It’s because for high-cost medicine, with complete costs within the hundreds of {dollars}, 15% coinsurance can translate into substantial out-of-pocket prices. For instance, partial LIS enrollees taking Humira or Enbrel for rheumatoid arthritis would pay round $1,900 for a 12 months’s value of those drugs in 2022, whereas full LIS enrollees would pay lower than $20 yearly. Thus, financial savings for partial LIS enrollees could be roughly $1,900 on value sharing for one among these drugs alone. Annual financial savings could be related for different high-cost specialty medicine, with nearly all of financial savings occurring under the catastrophic threshold the place partial LIS enrollees at the moment pay 15% coinsurance however full LIS enrollees pay low flat copays for brand-name medicine of both $3.95 or $9.85, relying on their earnings and asset ranges.
budgetary affect
CBO estimates that this provision will enhance federal spending by $2.2 billion over 10 years (2022-2031).
Additional Delay Implementation of the Trump Administration’s Drug Rebate Rule
provision description
The Inflation Discount Act additional delays implementation of the November 2020 remaining rule issued by the Trump Administration that might have eradicated rebates negotiated between drug producers and pharmacy profit managers (PBMs) or well being plan sponsors in Medicare Half D by eradicating the secure harbor safety at the moment prolonged to those rebate preparations beneath the federal anti-kickback statute. This rule was slated to take impact on January 1, 2022, however the Biden Administration delayed implementation to 2023, the Infrastructure Funding and Jobs Act signed into legislation on November 15, 2021 delayed implementation to 2026, and the Bipartisan Safer Communities Act signed into legislation on June 25, 2022 included an additional delay to 2027.
Efficient Date
This provision takes impact in 2027, delaying implementation of the rebate rule till 2032.
Individuals affected
Because the rebate rule by no means took impact, delaying it’s not anticipated to have a fabric affect on Medicare beneficiaries. Had the rule taken impact, it was anticipated to extend premiums for Medicare Half D enrollees, in keeping with each CBO and the HHS Workplace of the Actuary (OACT). OACT estimated {that a} small group of beneficiaries who use medicine with vital producer rebates may have seen a considerable decline of their total out-of-pocket spending beneath the rule, assuming producers handed on worth reductions on the level of sale, however different beneficiaries would have confronted out-of-pocket value will increase.
budgetary affect
As a result of the rebate rule was finalized (though not applied), its value has been included in CBO’s baseline for federal spending. Subsequently, delaying implementation of the rebate rule is predicted to generate financial savings. CBO estimates financial savings of $122.2 billion from delaying implementation of the Trump Administration’s rebate rule between 2027 (when the Inflation Discount Act delay takes impact) and 2032. As well as, CBO estimated financial savings of $50.8 billion between 2023 and 2026 for the three-year delay of this rule included within the Infrastructure Funding and Jobs Act and financial savings of $20.9 billion in 2026 and 2027 for the one-year delay included within the Bipartisan Safer Communities Act. It’s because each CBO and Medicare’s actuaries estimated considerably larger Medicare spending over 10 years because of banning drug rebates beneath the Trump Administration’s rule – as much as $170 billion larger, in keeping with CBO, and as much as $196 billion larger, in keeping with the HHS Workplace of the Actuary (OACT).
This work was supported partly by Arnold Ventures. KFF maintains full editorial management over all of its coverage evaluation, polling, and journalism actions




{kind=link}