

Medicaid enrollment has elevated in the course of the coronavirus pandemic, a development that doubtless displays antagonistic financial results of the pandemic (together with elevated job and revenue loss) in addition to steady protection necessities from the Households First Coronavirus Response Act. This situation transient analyzes enrollment and spending developments associated to the Reasonably priced Care Act’s Medicaid enlargement forward of the pandemic and examines potential penalties of current enrollment will increase. Key findings embrace:
On condition that the current financial downturn has brought about many adults to lose employment and/or revenue, Medicaid enlargement enrollment and spending are more likely to develop at a quick tempo in the course of the pandemic. Estimates counsel that enlargement enrollment development has outpaced general Medicaid enrollment development from February to August 2020. This evaluation sheds mild on the potential federal and state obligations for that spending and relative value to Medicaid packages. Wanting forward, uncertainty stays concerning the long run course of the pandemic, the scope and size of federal fiscal reduction efforts, and potential state and federal coverage actions to broaden protection. |
Introduction
The coronavirus pandemic has generated each a public well being disaster and an financial disaster, with main implications for Medicaid enrollment, significantly among the many enlargement inhabitants. Many individuals who lose their jobs and well being protection in the course of the pandemic will qualify for Medicaid if their revenue falls beneath eligibility limits, and low-income adults residing in states which have expanded Medicaid underneath the ACA could have extra protection choices than these in states that haven’t expanded. These states present protection to the Medicaid enlargement group, which incorporates adults underneath age 65 with incomes at or beneath 138% of the federal poverty degree (FPL). (Medicaid enrollees who don’t qualify for protection underneath the enlargement are known as the “conventional Medicaid” group all through this transient; see Field 1 for extra particulars.) Medicaid enrollment has elevated by greater than 5 million people in the course of the pandemic from February to August 2020. Knowledge from a subset of states means that enrollment by way of the enlargement has outpaced development general because the begin of the pandemic.
Elevated Medicaid enrollment has implications for each federal and state spending. For conventional Medicaid enrollees, states obtain their common match charge (“FMAP”) plus further federal assist by way of a 6.2 share level improve within the federal Medicaid match charge for conventional Medicaid spending. The federal authorities continues to pay a bigger share (90%) of the prices for these already or newly enrolled within the enlargement group. New enlargement group enrollment is more likely to compose a big share of elevated general Medicaid enrollment in the course of the pandemic; nevertheless, the 6.2 share level FMAP improve doesn’t apply to spending for the enlargement group.
This situation transient analyzes pre-pandemic developments for enrollment in and spending on the enlargement group and examines potential penalties of current enrollment will increase in the course of the pandemic. Enrollment and expenditure knowledge are from the Medicaid Funds and Expenditure System (MBES). As of writing, enrollment knowledge for the fourth quarter of FY 2019 haven’t been launched, and our FY 2019 enrollment figures are drawn from annualized enrollment totals from the information out there. Moreover, two states, Maine and Virginia, carried out Medicaid enlargement later in FY 2019, so enlargement spending in these two states mirror solely the months that the enlargement has been in impact. States which have or plan to implement the enlargement after FY 2019 (Idaho, Utah, Nebraska, Oklahoma, and Missouri) are thought of non-expansion states for all years of this evaluation. Enrollment and expenditure knowledge for New York have been adjusted because of what look like reporting anomalies for the standard Medicaid group and enlargement group, which affected nationwide totals. We didn’t make changes for every other states. See the Strategies part for extra data.
| The Medicaid enlargement group consists of people who’re enrolled within the Medicaid enlargement underneath the ACA. In states which have carried out the Medicaid enlargement (which was made successfully elective by the Supreme Courtroom ruling on the ACA’s constitutionality), practically all adults underneath age 65 and with incomes at or beneath 138% of the FPL ($17,609 per 12 months for a person in 2020) are eligible for Medicaid. States obtain an enhanced federal match charge for spending on enlargement adults, though there was a distinct federal match charge for adults who grew to become newly eligible underneath the ACA (“newly eligible enrollees”) versus adults had been enrolled by way of state waivers previous to passage of the regulation in 2009 (“not newly eligible enrollees”). As of January 2020, the federal match charge for all Medicaid enlargement group spending is 90%, the place it can stay going ahead.
The normal Medicaid group consists of all different Medicaid enrollees not enrolled by way of the Medicaid enlargement. Past federally mandated eligibility teams, states have discretion by which teams are eligible for Medicaid protection, however these usually embrace qualifying kids, individuals with disabilities, pregnant ladies, aged people, folks dually enrolled in Medicaid and Medicare, and low-income mother and father with eligibility ranges at pre-ACA limits (the pre-ACA median eligibility restrict for fogeys throughout all states was 64% of the FPL). The federal match charge for this group is predicated on states’ lagged relative per capita revenue and, in FY 2019, ranged from a ground of fifty% to a excessive of 76%. |
Medicaid Growth Enrollment
In FY 2019, the enlargement group represented 20% of all Medicaid enrollment and 28% of enrollment in enlargement states (Determine 1, Appendix Desk 1). In whole, Medicaid enrollment for FY 2019 was 75.2 million people throughout all 50 states and DC, with 15.3 million adults enrolled within the enlargement group. Throughout the enlargement group, most (81%, 12.5 million) had been newly eligible enrollees lined by way of Medicaid enlargement, whereas a smaller share (19%, 2.9 million) weren’t newly eligible enrollees (childless adults who had been enrolled by way of state waivers previous to passage of the ACA). Nearly all of Medicaid enrollment general (80%, 59.8 million) was inside the conventional Medicaid group, which consists of a number of completely different eligibility teams (see Field 1 above for extra data). These teams are topic to various eligibility ranges throughout states, with kids and pregnant ladies typically lined at a lot increased eligibility ranges in comparison with non-expansion mother and father and seniors and folks with disabilities.
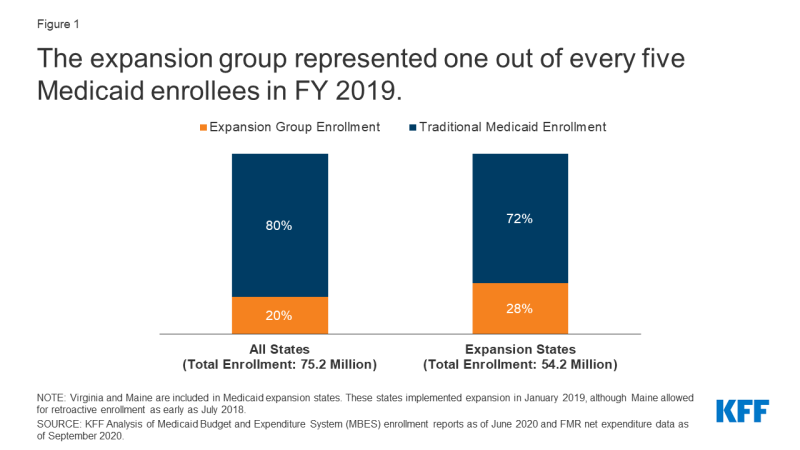
Determine 1: The enlargement group represented one out of each 5 Medicaid enrollees in FY 2019.
The share of Medicaid enrollment represented by the enlargement group varies throughout enlargement states in FY 2019 (Determine 2). Growth enrollment ranged from a excessive of 48% of whole enrollment in Oregon to a low of 11% in Maine, which carried out Medicaid enlargement protection within the second quarter of FY 2019 (January 2019), though Maine allowed for retroactive enrollment as early as July 2018. The variation throughout enlargement states doubtless displays a number of elements, together with completely different poverty distributions and financial circumstances throughout states (significantly, the state share of the inhabitants with revenue at or beneath 138% of the FPL) in addition to variation in state Medicaid eligibility ranges for enlargement and conventional teams. For instance, the District of Columbia covers enlargement adults above the minimal threshold of 138% FPL, with a threshold of 221% FPL for fogeys and 215% FPL for different adults.
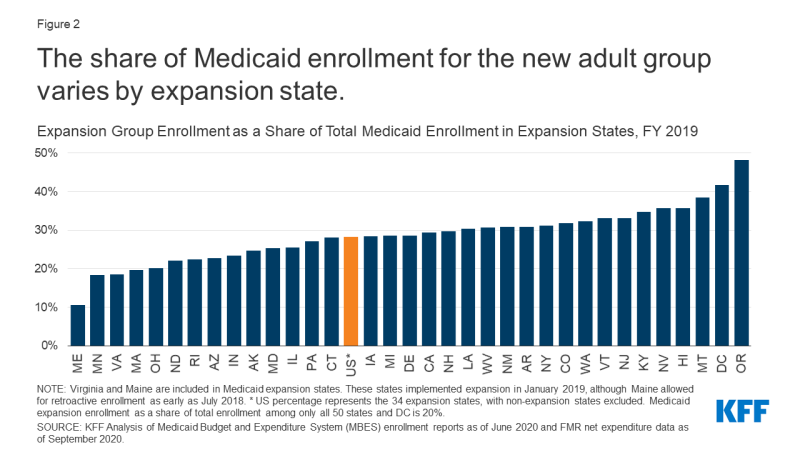
Determine 2: The share of Medicaid enrollment for the brand new grownup group varies by enlargement state.
Growth group enrollment peaked in FY 2017 and FY 2018 however declined in FY 2019, regardless of two states (Maine and Virginia) that newly carried out Medicaid enlargement that 12 months (Determine 3). Growth enrollment grew from 13.6 million enrollees in FY 2015 (the primary full fiscal 12 months of Medicaid enlargement following its implementation starting January 2014), when 30 states had carried out enlargement, and peaked at roughly 15.6 million enlargement enrollees in FY 2017 and FY 2018, when 32 states had carried out enlargement. Growth enrollment declined to fifteen.3 million in FY 2019, regardless of the addition of two extra states implementing enlargement that 12 months (34 in all). Conventional Medicaid enrollment confirmed a distinct development, declining from a excessive of 63.2 million in FY 2015 to 59.8 million in FY 2019, with annual declines in all years besides FY 2018. Traits in general (conventional plus enlargement) Medicaid enrollment had been just like these for conventional Medicaid enrollment, with annual declines in yearly apart from FY 2018. A number of elements may have contributed to current declining enrollment for enlargement and conventional enrollees, equivalent to bettering financial circumstances, boundaries to sustaining or renewing protection, and federal funding cuts to outreach and enrollment packages that help eligible people enrolling in Medicaid or market protection.
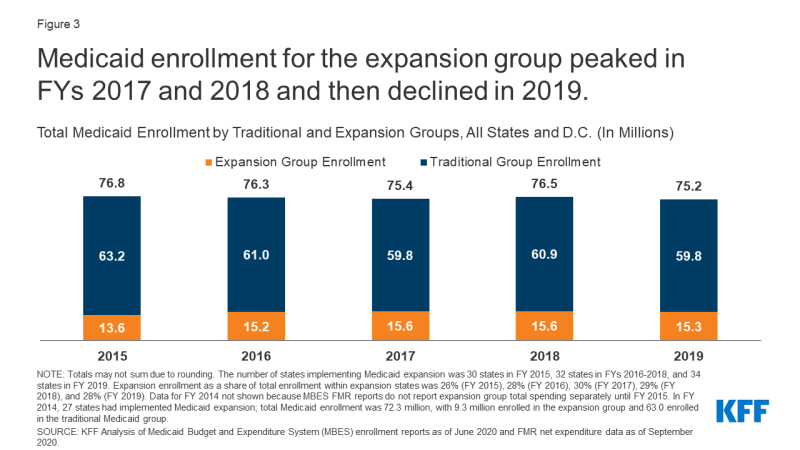
Determine 3: Medicaid enrollment for the enlargement group peaked in FYs 2017 and 2018 after which declined in 2019.
Medicaid Growth Spending
In FY 2019, spending on the enlargement group represented 16% of all Medicaid spending and 21% of spending in enlargement states (Determine 4, Appendix Desk 2). Medicaid spending totaled $594.6 billion throughout all 50 states and DC. Throughout the 34 states that carried out enlargement earlier than or throughout FY 2019, spending on the enlargement group totaled $93.8 billion that 12 months. Spending on the standard Medicaid inhabitants was a lot increased: $347.6 billion in enlargement states (79% of whole spending) and $500.8 billion throughout all states (84% of whole spending). This distinction in spending is partially defined by the larger variety of conventional enrollees in comparison with enlargement enrollees. Additional, the standard Medicaid group consists of many alternative eligibility teams, together with teams with smaller enrollment ranges however increased per-enrollee spending equivalent to seniors and folks with disabilities (for extra particulars, see Per Capita Spending part beneath). Thus, the proportion of spending represented by the enlargement group is decrease than its share of enrollment (21% vs. 28% in enlargement states).
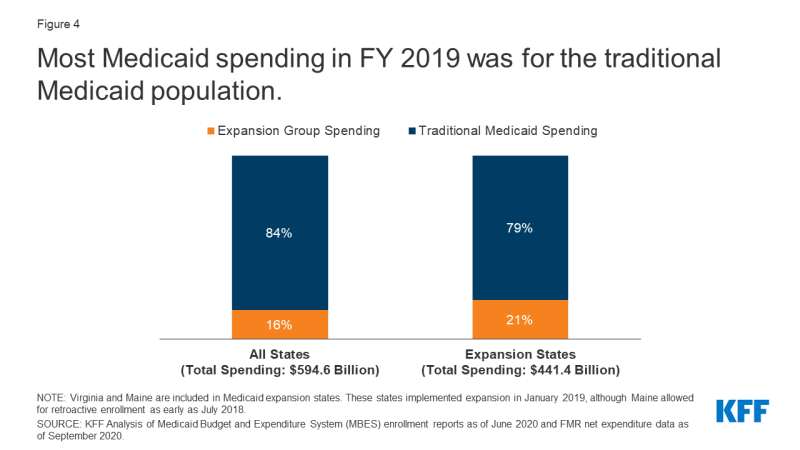
Determine 4: Most Medicaid spending in FY 2019 was for the standard Medicaid inhabitants.
The share of Medicaid spending represented by enlargement spending diversified throughout enlargement states in FY 2019 and was lower than 40% of whole spending in all these states (Determine 5). The share of spending on the enlargement group ranged from 4% in Maine to 39% in Montana. (Virginia and Maine carried out enlargement within the second quarter of FY 2019 and don’t characterize a full 12 months of spending.) Very like enrollment, a number of elements doubtless contribute to this variation. These embrace demographic variations throughout states (equivalent to age and revenue degree of the inhabitants), variation in profit packages and fee ranges, and state variation in eligibility limits for different, non-expansion teams (equivalent to seniors and folks with disabilities and oldsters with revenue at or beneath pre-ACA eligibility limits).
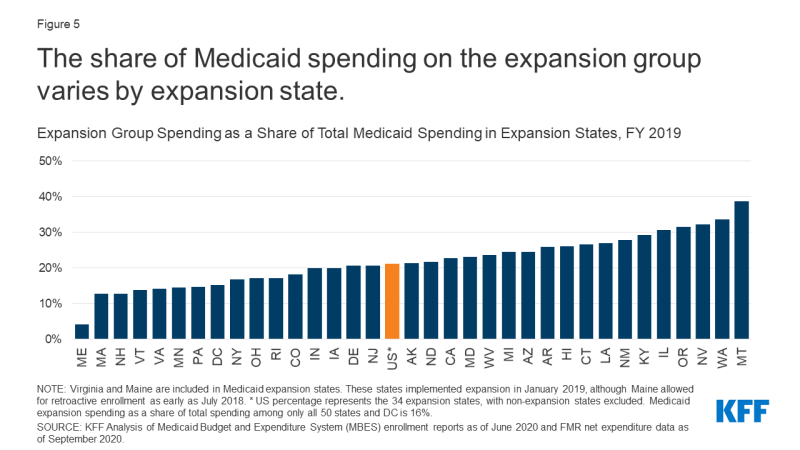
Determine 5: The share of Medicaid spending on the enlargement group varies by enlargement state.
Medicaid enlargement spending is primarily federal funds, with state spending on the enlargement group representing simply 1% of general Medicaid spending in FY 2019 (Determine 6). The ACA initially supplied 100% federal financing for enlargement prices in 2014; this match charge progressively fell to 93% in 2019 then to 90% in 2020 and past. In FY 2019, enlargement spending totaled $93.8 million, $84.9 billion of which was paid for by the federal authorities with the remaining $8.9 billion paid for by states. In distinction, states contributed a bigger proportion of conventional Medicaid spending, attributable to the decrease federal match charge for the standard inhabitants, which in FY 2019 ranged from 50% to 76% primarily based on a statutory formulation that accounts for every state’s common per capita revenue relative to the nationwide common.
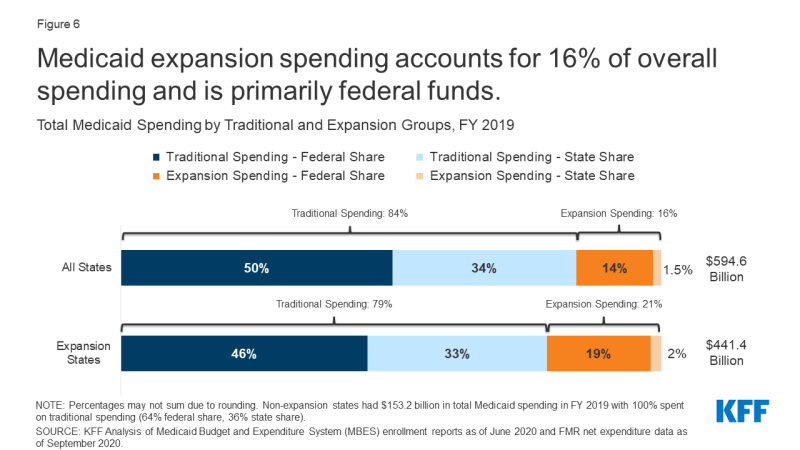
Determine 6: Medicaid enlargement spending accounts for 16% of general spending and is primarily federal funds.
As whole Medicaid spending has elevated within the years since FY 2015, the share of spending represented by the enlargement group has remained practically fixed (Determine 7). The share of Medicaid spending on the enlargement group has remained between 20% and 22% of whole Medicaid spending in enlargement states for yearly from FY 2015 by way of FY 2019, suggesting that will increase in whole Medicaid spending over these years have been proportionately pushed by the enlargement and conventional populations. The share of whole spending represented by enlargement spending has remained equally fixed throughout all states as nicely (between 14% and 16%). Notably, whereas whole spending elevated in FY 2019 for each the enlargement and conventional Medicaid teams, enrollment declined that 12 months. Not accounting for the preliminary improve in spending instantly following implementation, enlargement states and non-expansion states skilled related whole spending development from FY 2015 to FY 2019: 12% development for each the 30 states that expanded Medicaid by FY 2015 (excluding Louisiana, Maine, Montana, and Virginia, which carried out enlargement between FY 2015 and FY 2019) in addition to for the 17 non-expansion states. A number of elements might clarify rising Medicaid prices other than enrollment, together with adjustments to the make-up of the Medicaid inhabitants, service utilization, and rising prices. In FY 2019, states recognized growing prices for pharmaceuticals, supplier charge will increase, pressures from an getting older inhabitants, and the next acuity case-mix as key upward pressures on whole Medicaid spending.
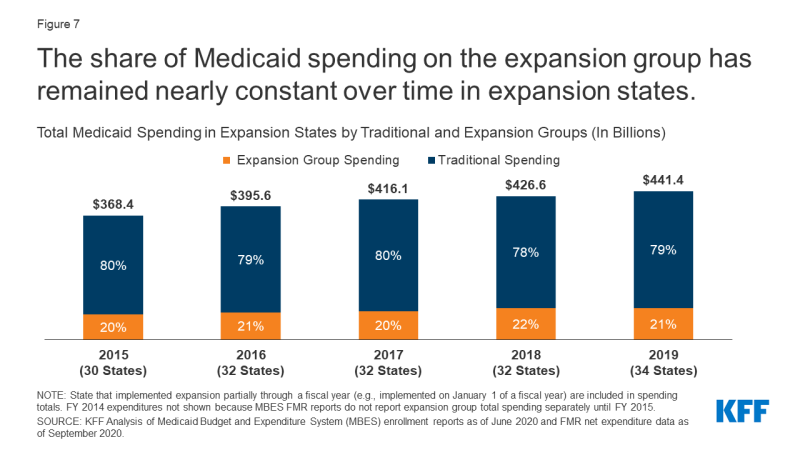
Determine 7: The share of Medicaid spending on the enlargement group has remained practically fixed over time in enlargement states.
Per Capita Spending
Medicaid spending per enrollee is decrease for the enlargement group than for different teams (Determine 8, Appendix Desk 3). Whereas general spending per enrollee was $7,910 in FY 2019, spending per enlargement enrollee was simply $6,110 and spending per conventional enrollee was $8,370 (spending per enlargement enrollee could also be barely underreported because of Maine and Virginia implementing enlargement later on this fiscal 12 months). This distinction is in step with earlier knowledge discovering decrease spending per enrollee for adults and youngsters as in comparison with different teams. In distinction, the aged and beneficiaries with disabilities account for a disproportionate share of Medicaid spending, largely attributable to larger want for acute care and long-term care.
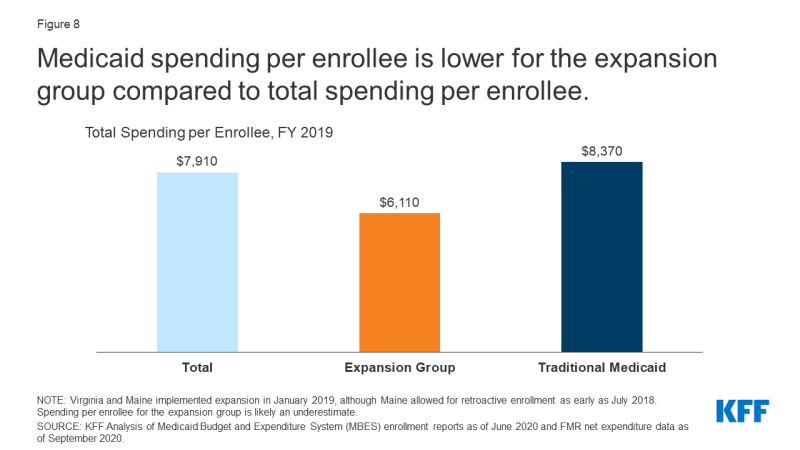
Determine 8: Medicaid spending per enrollee is decrease for the enlargement group in comparison with whole spending per enrollee.
Spending per enlargement enrollee varies throughout enlargement states (Determine 9). In FY 2019, spending per enlargement enrollee ranged from $3,950 in Vermont to $12,330 in North Dakota (Virginia and Maine carried out enlargement within the second quarter of FY 2019, so spending per enlargement enrollee could also be barely underreported in these figures). Spending per enlargement enrollee was decrease than per capita spending for different teams in practically all enlargement states, and states with increased whole spending per enrollee typically additionally had increased spending per enlargement enrollee. Elements which will contribute to variation in per capita spending throughout states embrace variations in well being care prices and utilization and the relative well being standing of the underlying populations.
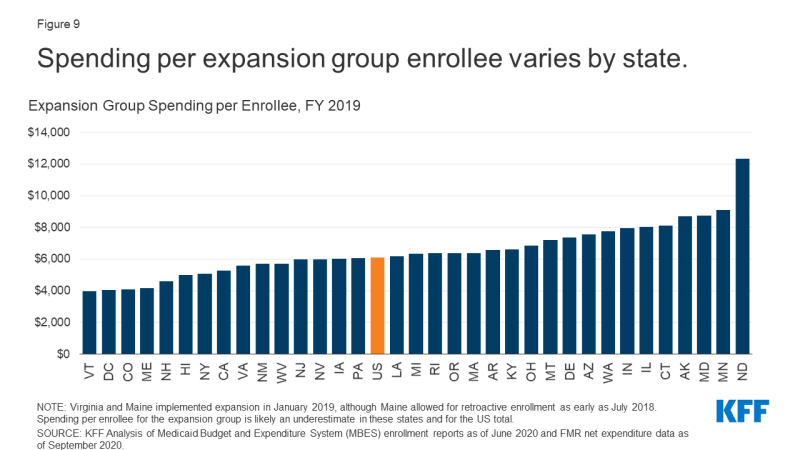
Determine 9: Spending per enlargement group enrollee varies by state.
Wanting Forward
Medicaid enlargement enrollment has grown at a quick charge in the course of the pandemic. In a reversal of prior developments, current knowledge reveals that whole enrollment is growing in the course of the pandemic, reflecting adjustments within the financial system (as extra folks expertise revenue and job loss and turn out to be eligible and enroll in Medicaid protection) and provisions within the Households First Coronavirus Response Act (FFCRA) that require states to make sure steady protection for present Medicaid enrollees and meet different upkeep of eligibility (MOE) circumstances to entry a short lived improve within the Medicaid federal match charge. Present Medicaid and CHIP enrollment knowledge present that whole enrollment elevated by over 5 million (7.4%) from February to August 2020, with non-expansion states experiencing barely sooner development over this time interval as in comparison with enlargement states (8.4% development vs. 7.1% development). Nonetheless, enrollment knowledge collected from a subset of state web sites for particular eligibility teams present that Medicaid enlargement enrollment is rising at a sooner charge than enrollment general, which might result in a commensurate improve in enlargement spending. Non-expansion states usually tend to see will increase within the uninsured inhabitants as adults who lose employer-sponsored insurance coverage in the course of the pandemic have fewer protection choices in these states.
Though federal {dollars} pays for almost all of elevated Medicaid spending in the course of the pandemic, states nonetheless face financial stress and will look to value chopping measures. The federal authorities pays 90% of prices for the enlargement group, which is considerably increased than the common match charge in all states. Moreover, analysis displaying optimistic financial outcomes from the Medicaid enlargement means that enlargement states might be higher positioned to deal with the financial fallout of the pandemic. The federal authorities additionally continues to contribute the next portion of non-expansion spending to offset prices in the course of the pandemic: underneath the FFCRA, states that meet MOE circumstances obtain a further 6.2 share level improve within the federal match charge for conventional spending by way of the quarter by which the nationwide public well being emergency declaration ends. Regardless of substantial will increase in federal {dollars} going to states for Medicaid in the course of the pandemic, budgetary pressures might trigger some states to look to Medicaid program cuts. Due to the federal match for Medicaid spending, programmatic cuts have to be substantial to generate state financial savings, particularly for the enlargement inhabitants. For instance, a $100 discount in enlargement spending would yield solely $10 in state financial savings.
Wanting forward, uncertainty stays concerning the long run course of the pandemic, the scope and size of federal fiscal reduction efforts, and potential state and federal coverage actions to broaden protection. As folks proceed to lose jobs and revenue in the course of the pandemic, non-expansion states might take into account adopting Medicaid enlargement to extend protection. Whereas any new adoption of enlargement would improve federal {dollars} going to states because of the 90% federal match, states might have problem overlaying the remaining 10% of enlargement spending amid antagonistic state budgetary impacts in the course of the pandemic. On the federal degree, President-elect Joe Biden has supported a brand new federal public medical health insurance choice which might be out there to people in non-expansion states who would in any other case be eligible had their states adopted Medicaid enlargement; nevertheless, this plan might face challenges to passage in a intently divided Senate. Policymakers might take into account extra slim choices, equivalent to proposals to make 100% federal financing out there to states that newly broaden. Moreover, President-elect Joe Biden may implement plenty of administrative actions that might improve Medicaid protection in enlargement and non-expansion states
| This evaluation makes use of knowledge from the Medicaid Funds and Expenditure System (MBES) from the Facilities for Medicare and Medicaid Providers (CMS). MBES enrollment knowledge might differ from different Medicaid enrollment counts, such because the Medicaid and CHIP Efficiency Indicator Challenge. MBES enrollment knowledge are reported month-to-month and primarily based on an unduplicated rely of people enrolled in Medicaid at any time within the month. Moreover, enrollment knowledge embrace people enrolled in restricted profit plans. Enrollment knowledge for the fourth quarter of FY 2019 haven’t been launched as of writing, and enrollment figures offered on this transient for FY 2019 are primarily based on annualized measures of the primary three quarters of the 2019 fiscal 12 months, described instantly beneath. MBES expenditure knowledge for FY 2019 are full for the total fiscal 12 months.
Fiscal 12 months Enrollment: Annual enrollment totals used on this report are primarily based on the utmost month-to-month enrollment for the fiscal 12 months in every state. Whereas this measure is used to estimate the full variety of enrollees over your complete fiscal 12 months, it’s doubtless an undercount of the variety of enrollees served all year long. Complete Medicaid enrollment is calculated from the utmost month-to-month whole enrollment. Medicaid enlargement group enrollment is calculated because the sum of the utmost newly eligible enlargement Group VIII enrollment and the utmost not newly eligible Group VIII enrollment reported in MBES, in step with a earlier KFF evaluation (Group VIII is synonymous with the enlargement group outlined on this report). Conventional Medicaid enrollment is calculated because the distinction between the utmost month-to-month whole enrollment for a fiscal 12 months and the Medicaid enlargement group whole. Conventional Medicaid enrollment and enlargement group enrollment sum to whole enrollment for every fiscal 12 months. Nationwide totals are the sum of states’ enrollment totals. Fiscal 12 months Expenditures: Expenditure totals for states are extracted from annual Monetary Administration Stories (FMR). Nationwide totals characterize the sum of state totals. Growth States: States with Group VIII enrollment of a minimum of one enrollee in a fiscal 12 months are thought of enlargement states in that 12 months for this evaluation. In FY 2019, this consists of all states which had carried out the enlargement by September 30, 2019 and excludes states which have carried out or plan to implement the enlargement after this date (Idaho, Utah, Nebraska, Oklahoma, and Missouri). Protection underneath the ACA’s Medicaid enlargement grew to become efficient January 1, 2014 (partway by way of FY 2015) in most states, with further states implementing enlargement after this date. State enlargement implementation dates might not align with federal fiscal years, and we didn’t modify our calculations for enlargement enrollment or expenditures for states that carried out enlargement later within the fiscal 12 months. In 2019, this solely affected Maine and Virginia, which each carried out enlargement on January 1, 2020, with Maine permitting retroactive enrollment by way of July 2018. Adjusting enlargement enrollment to mirror three-quarters of the fiscal 12 months in these two states didn’t make a big distinction for nationwide totals. Growth spending in these two states mirror solely the months that the enlargement was in impact. Changes: Resulting from what look like knowledge reporting anomalies in expenditures for the standard Medicaid group and the enlargement group (doubtlessly reflecting changes and recategorizations) that affected nationwide totals, New York expenditures for FY 2017 by way of FY 2019 had been adjusted by making use of the spending distribution for these teams from FY 2016. Complete Medicaid spending for New York was not adjusted. We additionally excluded enrollment knowledge from the third and fourth quarters of FY 2017 for New York, because of anomalous, massive shifts in enrollment between the standard Medicaid group and the enlargement teams. Complete enrollment was constant by way of FY 2017, indicating that no massive adjustments in enrollment for both conventional or enlargement teams doubtless occurred within the quarters that we excluded. |






{kind=link}