
Within the face of rising prescription drug prices, a big majority of the general public helps federal efforts to decrease drug spending. In his 2022 State of the Union deal with, President Biden urged Congress to move laws to rein in drug prices. In November 2021, the Home of Representatives handed the Construct Again Higher Act (BBBA), which incorporates a number of provisions that might decrease prescription drug prices, however the Senate has but to take motion on this laws. Proposals included within the BBBA would enable the federal authorities to barter the worth of some medicine lined beneath Medicare Half B (medicine administered by physicians and different well being care suppliers) and Half D (retail prescribed drugs); require drug corporations to pay rebates to the federal authorities when annual will increase in drug costs for Medicare and personal insurance coverage exceed the speed of inflation; cap month-to-month insulin prices for individuals with Medicare and personal insurance coverage; and cap Medicare beneficiaries’ out-of-pocket drug spending beneath Half D (however not Half B).
To higher perceive the potential out-of-pocket price publicity that Medicare beneficiaries might face for Half B medicine, on this transient we analyze cost-sharing legal responsibility for these medicine in conventional Medicare and cost-sharing necessities in Medicare Benefit plans. Information limitations preclude us from analyzing precise out-of-pocket prices paid by beneficiaries who used Half B medicine. For conventional Medicare beneficiaries, claims knowledge don’t report individually cost-sharing legal responsibility paid immediately by beneficiaries versus supplemental insurance coverage (the place relevant). For Medicare Benefit enrollees, there are not any knowledge accessible on precise out-of-pocket prices paid for Half B medicine.
Beneficiaries in conventional Medicare are charged 20% of the price of Half B medicine, with no annual restrict on their out-of-pocket prices. Beneficiaries enrolled in Medicare Benefit plans – which account for a rising share of the Medicare inhabitants and presently cowl near half of all beneficiaries – additionally usually face cost-sharing necessities for Half B medicine as much as their plan’s out-of-pocket restrict ($7,550 for in-network price sharing and $11,300 for in-network and out-of-network price sharing mixed in 2022). Most however not all beneficiaries in conventional Medicare have some type of supplemental protection to assist with their Medicare cost-sharing necessities, whereas most Medicare Benefit enrollees don’t. For instance, most conventional beneficiaries who’ve Medigap have a coverage that covers the 20% coinsurance for Half B medicine and providers, whereas Medicaid and a number of the Medicare Financial savings Packages cowl Medicare price sharing for eligible low-income beneficiaries in each conventional Medicare and Medicare Benefit. However even these with supplemental insurance coverage might face some out-of-pocket prices for his or her Half B medicine, relying on the generosity of their protection. As well as, roughly 6 million Medicare beneficiaries don’t have any supplemental protection and could be accountable for the complete 20% coinsurance.
Within the first a part of this evaluation, we study Medicare claims knowledge for 2019 to evaluate cost-sharing legal responsibility for Half B medicine for beneficiaries in conventional Medicare (excluding Half B vaccines since these are supplied without charge to Medicare beneficiaries). Within the second a part of our evaluation, we use Medicare Benefit profit design knowledge for 2022 to look at the vary in cost-sharing quantities at or under 20% coinsurance charged by Medicare Benefit plans for in-network Half B medicine. We additionally analyze variation in cost-sharing quantities for out-of-network Half B medicine charged by plans that present out-of-network protection. (See Strategies for added particulars on each elements of our evaluation.)
Findings
One-fourth of the 4.1 million conventional Medicare beneficiaries who used a number of Half B medicine in 2019 had common annual cost-sharing legal responsibility of not less than $1,000
Of the 4.1 million beneficiaries in conventional Medicare who acquired a number of Medicare Half B medicine included on this evaluation, 1 in 4 (1.0 million beneficiaries) confronted cost-sharing legal responsibility of not less than $1,000 and almost 1 in 5 (0.7 million) confronted cost-sharing legal responsibility of not less than $2,000 in 2019 (Determine 1). About 0.4 million conventional Medicare beneficiaries – or 1 in 10 of those that used Half B medicine – had not less than $5,000 in cost-sharing legal responsibility for these medicine in 2019. As beforehand famous, we’re unable to investigate what number of beneficiaries had supplemental insurance coverage to cowl some or all of those prices and what number of have been accountable for paying the complete quantity out-of-pocket.
For greater than half of all Half B medicine included on this evaluation, common annual cost-sharing legal responsibility was $1,000 or extra in 2019
Of the 287 Half B medicine included on this evaluation, greater than half (54% or 155 medicine) had common annual cost-sharing legal responsibility of not less than $1,000 in 2019, and greater than 4 in 10 (43% or 123 medicine) had cost-sharing legal responsibility of not less than $2,000.
- Eight of the highest 10 Half B medicine with the very best whole spending, and 18 of the highest 20, had common annual cost-sharing legal responsibility of not less than $1,000 in 2019 (Determine 2, Desk 1). For instance, common beneficiary legal responsibility for Eylea, the top-spending Half B drug in 2019 utilized by 270,300 conventional Medicare beneficiaries to deal with macular degeneration, was $2,100. For the most cancers drug Keytruda, second when it comes to whole Medicare Half B spending, common cost-sharing legal responsibility was $9,100.
- Conversely, common annual cost-sharing legal responsibility for a lot of the Half B medicine with the very best variety of customers was under $1,000. Solely 2 of the highest 10 Half B medicine based mostly on the variety of customers, and 4 of the highest 20, had common annual cost-sharing legal responsibility of not less than $1,000 in 2019 (Desk 2). For instance, common beneficiary legal responsibility for the most-commonly used (non-vaccine) Half B drug, Prolia (and the equal model Xgeva), an osteoporosis therapy utilized by almost 600,000 conventional Medicare beneficiaries in 2019, was $600.
Common annual cost-sharing legal responsibility exceeded $10,000 for greater than 1 in 10 Half B medicine on this evaluation (13% or 36 medicine). Whereas a number of the highest-liability medicine have been utilized by comparatively few beneficiaries to deal with uncommon circumstances, two of those medicine have been utilized by greater than 10,000 beneficiaries in 2019: Opdivo, a therapy for a number of sorts of most cancers utilized by 30,300 beneficiaries, with common annual cost-sharing legal responsibility of $10,200; and Darzalex, a therapy for a number of myeloma utilized by almost 12,000 beneficiaries, with common annual cost-sharing legal responsibility of $12,900.
Like beneficiaries in conventional Medicare, Medicare Benefit enrollees usually face 20% coinsurance for Half B medicine, however will be uncovered to increased cost-sharing necessities for these medicine when administered by an out-of-network supplier
Medicare Benefit plans have flexibility to find out cost-sharing quantities for Half B lined medicine, topic to sure limits, and may differentiate price sharing for chemotherapy from different Half B medicine. In 2022, Medicare Benefit plans are prohibited from charging greater than 20% coinsurance, or the equal copay quantity, for each chemotherapy and different Half B medicine from in-network suppliers. There are not any comparable restrictions on out-of-network cost-sharing quantities.
Based mostly on our evaluation of Medicare Benefit plan cost-sharing necessities and enrollment as of January 2022:
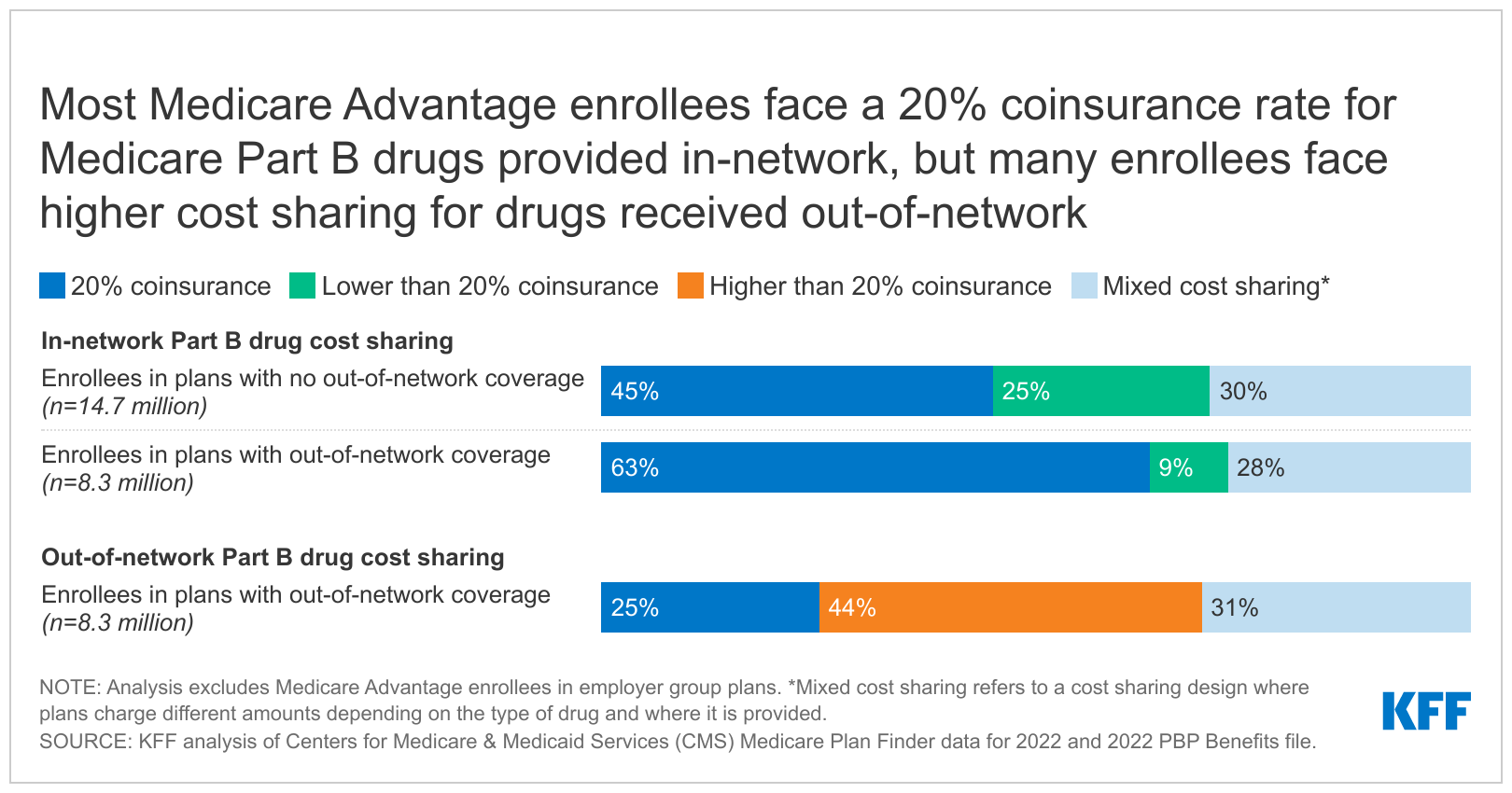
- According to present necessities, all 22.9 million Medicare Benefit enrollees included on this evaluation (excluding enrollees in employer group plans) face coinsurance of 20% or much less (or equal price sharing) for chemotherapy and different Half B medicine when supplied in-network (Determine 3). Some Medicare Benefit plans at all times cost lower than 20% coinsurance for each sorts of medicine; for instance, 25% of HMO enrollees and 9% of PPO enrollees and different plans that supply out-of-network protection cost lower than 20% coinsurance for Half B medicine administered in community. Different plans fluctuate cost-sharing quantities for Half B medicine (e.g., a $0 copayment or 20% coinsurance) relying on the kind of drug (e.g., chemotherapy vs. different Half B medicine) and/or the place it’s furnished (e.g., a pharmacy or different supplier setting).
- Among the many 8.3 million Medicare Benefit enrollees in PPOs and different sorts of plans with out-of-network protection, one-fourth of those enrollees (2.1 million) face 20% coinsurance for Half B medicine acquired from an out-of-network supplier, whereas near half (44% or 3.7 million) could be charged greater than 20% for these medicine if administered by an out-of-network supplier (Determine 4). Amongst these enrollees, 1.1 million are in plans that cost 50% for out-of-network Half B medicine, 1.1 million are in plans that cost 40% coinsurance, and 0.9 million enrollees are in plans that cost a 30% coinsurance (0.9 million). One other 31% of enrollees with out-of-network protection (2.5 million) might face coinsurance increased than 20% relying on the kind of drug and/or the place the drug is run.
- The 14.7 million Medicare Benefit enrollees in HMOs and different plans with no out-of-network protection would pay 100% of the associated fee for Half B medicine administered out-of-network until they acquired prior approval from their plan.
In contrast to conventional Medicare, Medicare Benefit plans have an out-of-pocket restrict, however Medicare Benefit enrollees can nonetheless face substantial cost-sharing quantities for a number of the higher-priced Half B medicine, particularly if administered out-of-network.
- For Eylea, a therapy for macular degeneration, Medicare Benefit enrollees would face common cost-sharing legal responsibility of $2,100 at a 20% coinsurance charge and as much as $5,200 at a 50% coinsurance charge, assuming the plan pays the identical worth as conventional Medicare.
- For Rituxan, a most cancers and autoimmune therapy, Medicare Benefit enrollees would face common cost-sharing legal responsibility of $4,600, based mostly on a 20% coinsurance charge for in-network chemotherapy, however might face prices as much as their plan’s most out-of-limit for this one drug alone based mostly on increased out-of-network coinsurance charges (as much as $11,300 in 2022).
- For Prolia (and the equal model Xgeva), an osteoporosis therapy, Medicare Benefit enrollees would face common cost-sharing legal responsibility of $600 at a 20% coinsurance charge and as much as $1,400 at a 50% coinsurance charge, assuming the plan pays the identical worth for these medicine as conventional Medicare.
Dialogue
Beneficiaries in each conventional Medicare and Medicare Benefit will be uncovered to probably excessive out-of-pocket prices for Half B medicine – although knowledge limitations preclude us from analyzing out-of-pocket prices paid immediately by beneficiaries who used Half B medicine in both conventional Medicare or Medicare Benefit plans and the share of prices lined by personal supplemental insurance coverage or Medicaid. We discover that, general, 1 in 4 beneficiaries in conventional Medicare who used Half B medicine in 2019 confronted cost-sharing legal responsibility of not less than $1,000, and greater than half of Half B medicine included on this evaluation had common cost-sharing legal responsibility of $1,000 or extra. Given the absence of an out-of-pocket restrict for beneficiaries in conventional Medicare, the prices of chemotherapy and different Half B medicine might signify a considerable monetary burden for beneficiaries with no supplemental protection, or with supplemental protection that doesn’t cowl all cost-sharing necessities for these medicine.
Whereas Medicare Benefit plans are required to have a most out-of-pocket restrict and may cost not more than 20% for Half B medicine administered by an in-network supplier, most Medicare Benefit enrollees would face increased prices for Half B medicine furnished by an out-of-network supplier, together with near 4 million enrollees in plans with out-of-network protection and almost 15 million enrollees in HMOs and different plans with no out-of-network protection. Plans with out-of-network protection usually cost increased price sharing for Half B medicine and different providers acquired out-of-network to encourage enrollees to obtain care from in-network suppliers the place plans have negotiated decrease costs. These community preparations and cost-sharing variations can have probably giant price implications for Medicare beneficiaries.
Among the many set of proposals that policymakers have just lately thought-about to decrease prescription drug prices, permitting the federal authorities to barter costs for some medicine lined beneath Half B and Half D and requiring inflation rebates for Medicare-covered medicine to restrict annual will increase in drug costs might assist to deal with the spending burden that Medicare beneficiaries might face in the event that they want high-cost medicine, whether or not lined beneath Half B or Half D.
This work was supported partially by Arnold Ventures. We worth our funders. KFF maintains full editorial management over all of its coverage evaluation, polling, and journalism actions.
| This evaluation relies on 2019 Medicare claims knowledge for individually payable (non-packaged) Half B medicine from a 20% pattern of Medicare beneficiaries, eradicating medicine taken by fewer than 11 beneficiaries within the pattern. The claims embody beneficiaries in conventional Medicare solely, excluding beneficiaries enrolled in Medicare Benefit. Utilizing HCPCS codes for Half B medicine, claims have been pulled from the outpatient, provider, and sturdy medical tools (DME) recordsdata, eradicating packaged medicine, vaccines, and claims from Maryland hospitals, Important Entry Hospitals, and dialysis services.
We calculate beneficiary legal responsibility utilizing variables within the claims knowledge similar to deductible and coinsurance quantities, however we aren’t in a position to decide the quantity {that a} beneficiary truly paid. Beneficiaries might not be accountable for some or all of their cost-sharing legal responsibility if they’ve sure sorts of supplemental protection, together with most Medigap insurance policies or full advantages by Medicaid. Medicare Benefit cost-sharing quantities and plan designs are based mostly on the Facilities for Medicare & Medicaid Companies (CMS) Medicare Plan Finder knowledge for 2022 and 2022 PBP Advantages file. Enrollment numbers are from the CMS January 2022 enrollment recordsdata. Plan-county enrollment and plan totals have been eliminated if fewer than 11 beneficiaries have been enrolled. Moreover, all employer plans have been faraway from the evaluation as they aren’t required to submit all the information obligatory for this evaluation. We additionally excluded all Medicare-Medicaid plans. For out-of-network Half B medicine in PPOs, knowledge limitations preclude us from assessing variations in out-of-network cost-sharing quantities for chemotherapy and different Half B medicine as a result of the Medicare Plan Finder doesn’t separate out-of-network price sharing for these two classes. It’s doubtless that the proportion of enrollees we report as having a combined cost-sharing construction for out-of-network Half B medicine could be decrease if the information allowed us to investigate out-of-network price sharing individually for chemotherapy and different Half B medicine. For an identical method, we estimated mixed in-network cost-sharing quantities based mostly on the quantities for chemotherapy and different Half B medicine. If these cost-sharing quantities have been analyzed individually, the proportion of enrollees paying 20% coinsurance could be increased for chemotherapy, with a decrease proportion of enrollees uncovered to a combined cost-sharing design. The odds for the separate class of different Half B medicine could be just like the odds we report for each chemotherapy and different Half B medicine mixed. |
Tables




{kind=link}