
Introduction
Entry to sexual and reproductive well being (SRH) care within the U.S. is influenced by quite a lot of elements, together with sufferers’ protection, social determinants of well being, in addition to federal, state, native, and institutional stage insurance policies. We have now additionally seen that well being care suppliers play a big function within the care sufferers obtain. To higher perceive how the availability of SRH care varies throughout the U.S., and the way supply of care has been influenced by adjustments in reproductive well being coverage, KFF performed a nationally consultant survey of OBGYNs throughout america. Whereas we acknowledge that many varieties of clinicians are vital sources of SRH care — from midwives, to advance follow clinicians to main care physicians— obstetrician-gynecologists (OBGYNs) comprise the most important subset of suppliers on this subject.
This survey requested OBGYNs about a variety of points, together with their provision of contraception, abortion, and STI care, the function of Medicaid within the supply of SRH, screening practices for psychosocial wants, and the affect of federal and state insurance policies on well being care high quality and entry.
Key Findings
Contraception:
- Almost all OBGYNs provided their sufferers some types of contraceptive care, however simply 18% of OBGYNs provided their sufferers all strategies of non-permanent contraception that have to be both prescribed or offered by a clinician. These strategies embrace the capsule, patch, ring, diaphragm or cervical cap, intrauterine gadgets (IUDs), contraceptive implants (Nexplanon), contraceptive injections (Depo-Provera) and emergency contraception (Copper IUD and Ulipristal Acetate/Ella). Those who provided all strategies tended to be youthful and work in giant practices, with greater than 10 clinicians.
- Whereas the overwhelming majority of OBGYNs offered each varieties of long-acting reversible contraception (LARCs) —IUDs (96%) and implants (84%— solely 4 in ten of those that offered these strategies provided same-day placement. Because of this on the majority of OBGYN practices, sufferers should make a couple of go to to acquire a LARC.
- Lower than half of OBGYNs reported that they offered prescription types of emergency contraception, which might forestall being pregnant after unprotected intercourse or within the occasion {that a} condom breaks. 45% offered the copper IUD and 42% offered Ella (the prescription “morning after capsule”). Almost 4 in ten reported that they don’t present both of those types of emergency contraception.
Abortion:
- Most OBGYNs (75%) reported their practices didn’t present abortions for being pregnant termination, however over one in 5 (23%) labored in practices that do. Abortion provision was extra frequent amongst OBGYNs in city and suburban areas in comparison with rural, and within the Northeast and West in comparison with the Midwest and South.
- Nearly all of OBGYNs who don’t supply abortions refer their sufferers to different suppliers for this service, however simply over one in ten (13%) neither present nor refer for abortions. Amongst those that don’t present abortions, essentially the most generally cited causes for not doing so included their follow having a coverage towards it (49%), saying that providers are available elsewhere (45%) and private opposition to the follow (31%). A better share of OBGYNs within the Midwest and South cited authorized rules as a purpose for not offering abortions, in comparison with these within the Northeast and West.
Different Sexual and Reproductive Well being Companies:
- The overwhelming majority of OBGYNs present onsite testing for gonorrhea and chlamydia (99%), syphilis (90%) and HIV (87%) at their practices. About half of OBGYNs mentioned they all the time or usually prescribe expedited associate remedy (EPT) for intercourse companions of sufferers with gonorrhea or chlamydia. Fewer than one in 5 (18%) prescribe pre-exposure prophylaxis (PrEP) for the prevention of HIV.
- A few quarter of OBGYNs (28%) work at practices that present gender affirming care, together with hormone remedy or gender affirming surgical procedure. Whereas the overwhelming majority of OBGYNs reported they felt considerably or very ready to fulfill the SRH wants of lesbian, homosexual, bisexual and queer sufferers (88%), simply over half felt the identical for transgender sufferers (56%).
- Screening for psychosocial wants diversified tremendously, with much more OBGYNs reporting they display screen all sufferers for intimate associate violence (70%) and despair (71%) than transportation (17%) and housing (19%) wants. Within the occasion of a constructive display screen, few OBGYNs mentioned that they had entry to sources onsite to deal with these wants.
Medicaid:
- Almost 4 out of 5 (78%) OBGYNs reported their follow accepts Medicaid. Many famous challenges related to offering take care of Medicaid sufferers, together with problem discovering specialists to simply accept referrals (73%), and being reimbursed at a decrease price than below non-public insurance coverage (90%).
- A sizeable minority mentioned that they had encountered no less than one Medicaid restriction relating to contraceptive care, together with needing to acquire prior authorization (45%), being restricted to an preliminary contraceptive provide of 30 days (33%), requiring “step-therapy” (15%) or being denied instant substitute of expelled or eliminated LARCs (15%).
Coverage Views:
- Many OBGYNs are conscious of the affect of out-of-pocket prices on their sufferers. About half of OBGYNs (53%) mentioned the problem of affordability comes up all the time or usually after they advocate checks or therapies to sufferers, and the same share of OBGYNs (53%) mentioned they have been all the time or usually conscious of the magnitude of their sufferers’ out-of-pocket prices. Almost all (92%) reported that the price of reproductive well being care poses a burden for low-income sufferers of their practices.
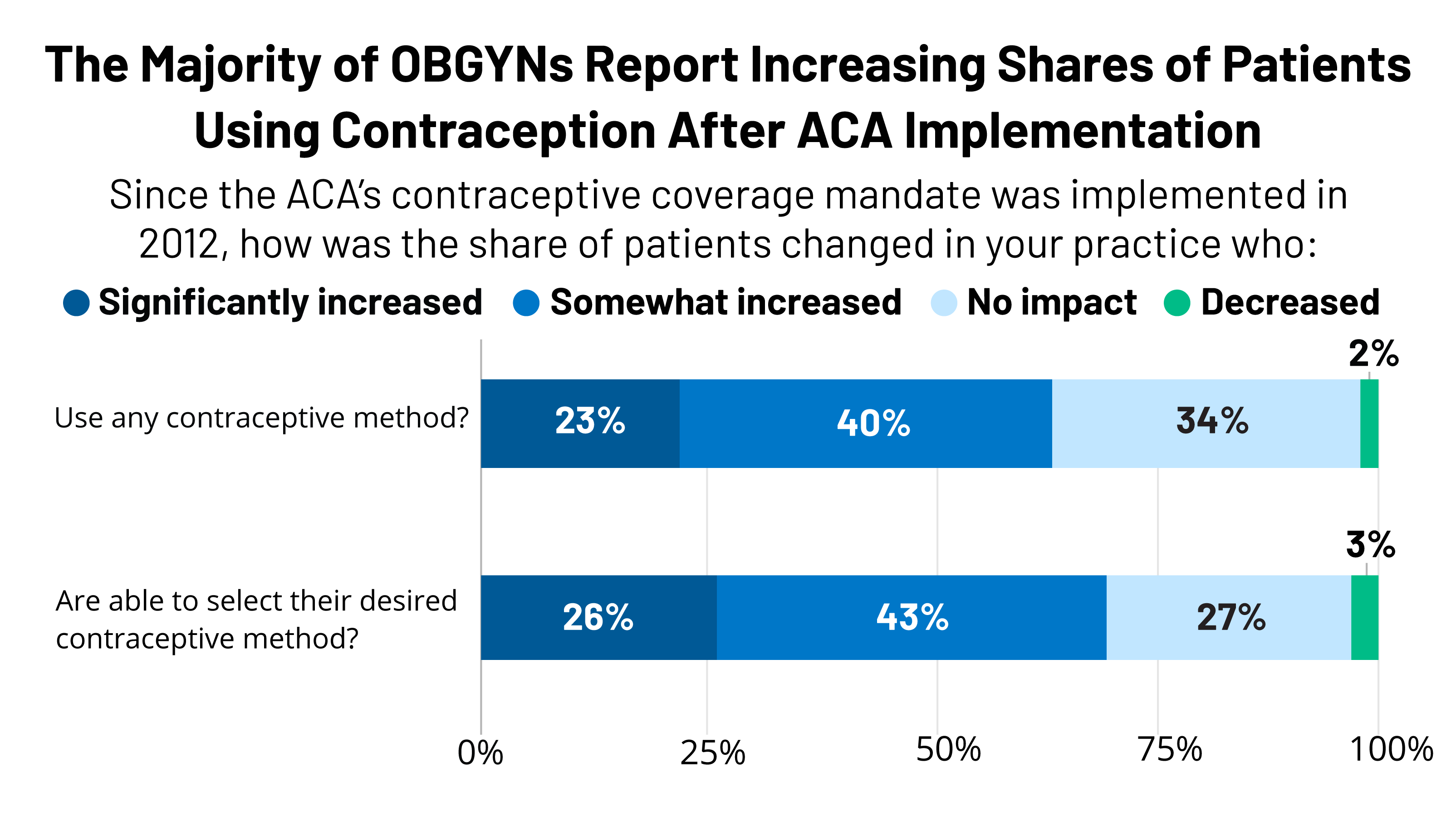
- Over six in ten OBGYNs reported a rise within the share of their sufferers who have been utilizing any contraceptive technique (63%) in addition to their desired contraceptive technique (69%) since implementation of the ACA’s contraceptive protection requirement in 2012.
- Over one in 4 (28%) reported that current state-level abortion rules together with gestational age limits and rules of suppliers have had a unfavourable affect on their potential to supply high quality reproductive well being care; the bulk (68%), nevertheless, reported that new abortion rules have had no affect on care. Solely 3% mentioned that they improved care.
- When requested about profession satisfaction, 70% of OBGYNs reported they’d select the identical medical specialty, whereas a minority mentioned they’d select a special specialty (19%) or not be a doctor in any respect (10%).
Conclusions and Implications
Our findings counsel that sufferers could expertise gaps within the availability of complete SRH care provision relying on the place they search care and the suppliers they see. The overwhelming majority of OBGYNs offered most types of hormonal contraception, STI testing, cervical most cancers screening, primary infertility diagnostics and prenatal care, however solely a minority offered emergency contraception, abortion care, PrEP for HIV prevention, gender affirming care and sources to deal with psychosocial wants. This will replicate variations in coaching, private preferences, and useful resource availability amongst OBGYNs.
Regional variation in SRH provision have been was noticed, notably relating to the provision of same-day LARC insertions, abortion provision, and preparedness to fulfill the wants of LGBTQ sufferers. This might counsel that variations in state-level insurance policies round SRH care, together with the choice to develop Medicaid or not, could also be influencing follow.
Variations in service provision have been additionally noticed by doctor age. Youthful physicians extra usually reported offering all strategies of contraception, same-day LARCs, PrEP for HIV prevention, prenatal care and gender affirming care in comparison with the oldest group of OBGYNs.
Throughout a number of measures, a extra complete array of SRH providers was accessible from OBGYNs who practiced in well being facilities/clinics quite than non-public office-based practices. Whereas the explanation for this distinction is unknown primarily based on this survey, it might maybe replicate adherence to pointers set out by the Well being Assets & Companies Administration’s Bureau of Main Well being Care Well being Heart Program and the Workplace of Inhabitants Affairs’ (OPA) High quality Household Planning Pointers. It’s notable that the overwhelming majority of OBGYNs reported they settle for Medicaid sufferers of their follow, and OBGYNs who served a big share of Medicaid sufferers had comparable follow patterns in comparison with those that don’t serve many Medicaid sufferers.
Most OBGYNs reported following reproductive well being coverage debates intently however had blended views on how well being coverage adjustments influenced their practices. For instance, most OBGYNs perceived will increase within the share of their sufferers utilizing contraception since implementation of the ACA contraceptive protection mandate, however a minority perceived any affect of current abortion rules on their potential to supply high quality reproductive well being care. This may very well be attributed to the sizable variation throughout the nation within the adoption of abortion restrictions in comparison with the affect of the ACA’s contraceptive requirement that affected most girls with non-public protection no matter their state of residence.
Total, we noticed heterogeneity during which SRH providers OBGYNs present, various by each doctor and follow traits. Gaps in SRH provision which were highlighted from this survey warrant consideration on the supplier, institutional and coverage stage, with a view to proceed to attempt for improved affected person outcomes and experiences.





{kind=link}