
Many individuals imagine that the US is a fee-for-service system and plenty of European international locations are extra seemingly to make use of world capitation reimbursement for suppliers. Those that dislike fee-for-service declare it incentivize over-treatment and disincentives prevention and use phrases like “waste” and “too costly”. Those that dislike world capitation declare that method results in diminished entry to care and longer wait occasions for care and phrases used embrace “rationing” and “queuing”. Nonetheless, the U.S. is dipping its toe in experimenting with world capitation.
One instance of world capitation fee within the US is the Pennsylvania Rural Well being Mannequin (PARHM). How does this system work? A current paper by Scanlon et al. (2022) explains:
The Pennsylvania Rural Well being Mannequin is a $25 million, 6-year demonstration funded by the Heart for Medicare and Medicaid Innovation (CMMI). In the end, the mannequin will take a look at whether or not world funds for the healthcare wants of a inhabitants will result in care supply transformation and improved high quality of care and decrease prices for rural Pennsylvanians.
Underneath the worldwide fee, individuals obtain the historic internet affected person income for inpatient and outpatient hospital providers for every collaborating payer. A part of the curiosity in world capitation was Maryland’s adoption of a world price range mannequin for 10 of its rural hospitals in 2010. This technique changed the earlier fee-for-service primarily based system.
A report evaluating the primary yr of this system explains the mannequin in additional element. PARM is multi-payer initiative, which incorporates participation from Medicare, business payers, business payers’ Medicaid managed care and Medicare Benefit plans.
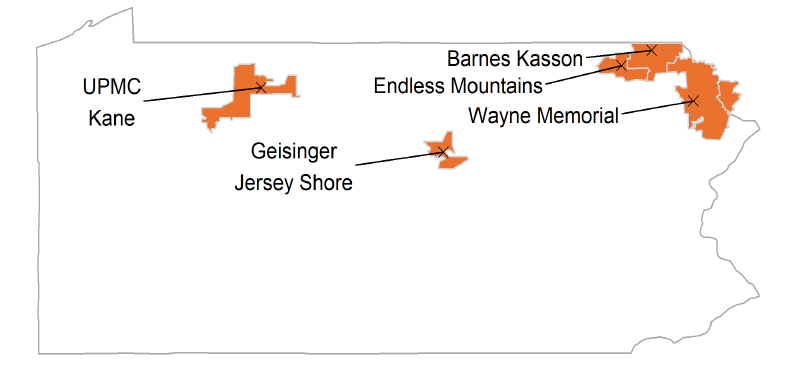
Which hospitals have joined this system?
On the time of the Mannequin announcement (2017), 67 rural hospitals, together with 15 [critical access hospitals] CAHs, have been eligible to take part within the Mannequin. 5 hospitals joined the Mannequin for PY1 (2019), eight extra hospitals joined the Mannequin for PY2 (2020), and 5 extra hospitals joined the Mannequin for PY3 (2021). Thus far, all individuals stay the Mannequin for PY3 (2021). Taking part business payers embrace 4 Pennsylvania-based payers and one nationwide insurer.
How have been the hospitals doing earlier than PARHM was applied and the way are they doing afterwards?
The short- and long-term monetary viability of the Cohort 1 hospitals worsened through the baseline interval [i.e., prior to PARHM]—a possible motivating issue for his or her participation within the PARHM. Declining inpatient quantity and glued prices might have negatively impacted monetary efficiency through the baseline interval…
[After the adoption of PARHM] Biweekly funds below the worldwide price range addresses variability in funds as a consequence of seasonality and quantity shifts. Hospitals perceived this as an essential Mannequin function. Throughout PY1 (2019), previous to ultimate reconciliation of Medicare reimbursements, interim world price range funds exceeded the interim Medicare reimbursement quantity the Cohort 1 hospitals would have been paid below FFS and cost-based reimbursement strategies.
Briefly rural hospitals seem like a bit higher off financially below PARHM. It will likely be fascinating to see how PARHM operated in a extra dynamic setting of the COVID-19 pandemic, the place prices and utilization are a lot tougher to foretell below a pandemic. On the one hand, world capitation might present hospitals monetary stability from shedding income from elective surgical procedures which have been deferred; then again, it’s unclear if PARHM–with out different monetary assist–would have offered sufficient compensation to assist COVID-19 pandemic associated actions.





{kind=link}